Original article
Craniocervical position characteristics for different occlusions in developing patients: Craniocervical relationship and occlusion
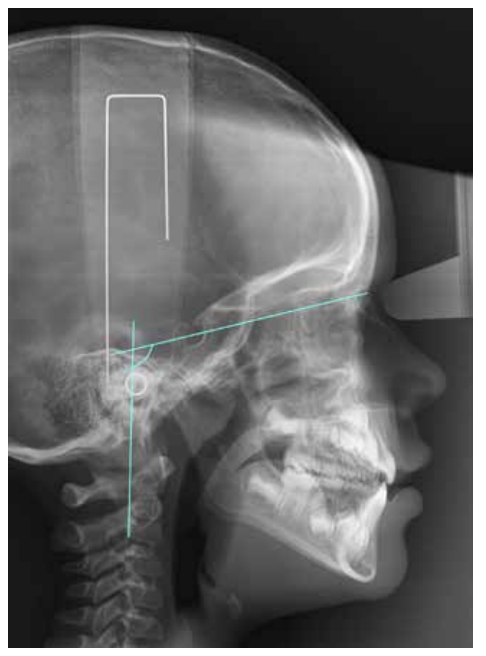
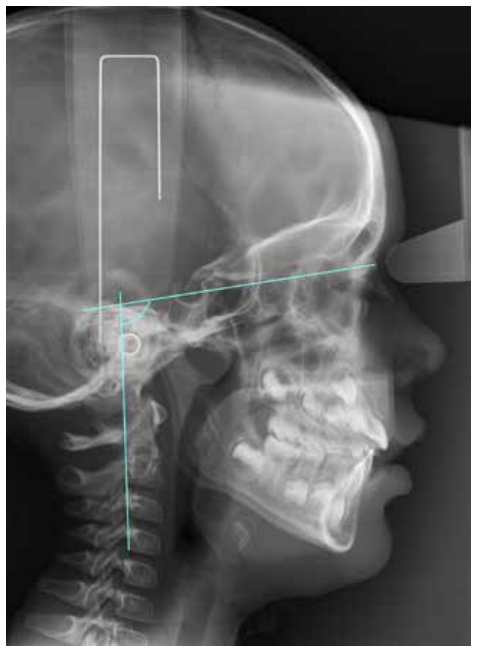
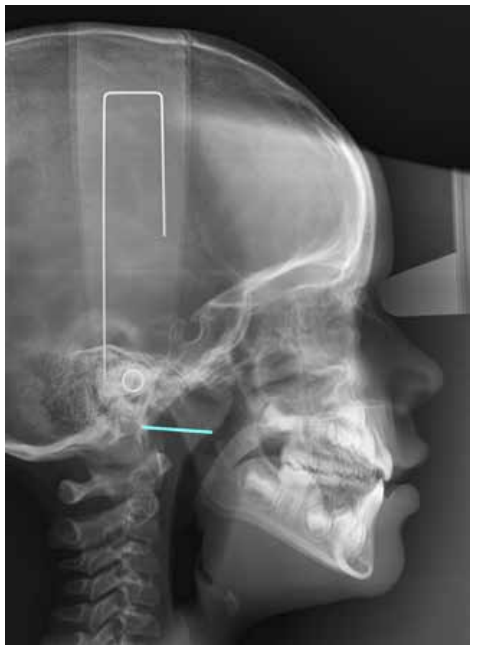
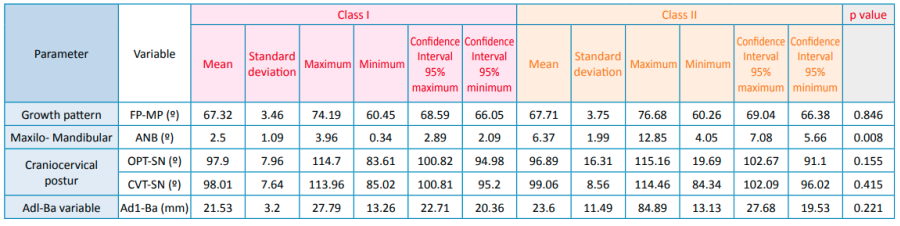
Currently, the relationship between occlusion and posture arouses great scientific interest, especially during the establishment of a multidisciplinary treatment. However, the diversity of studies refers mostly to the adult population and there is no common agreement among the different investigations. Based on this, we aimed to study the craniocervical position in different occlusions in the developing pediatric population. Through a crosssectional design, 64 pediatric patients with complete clinical history and highquality lateral skull radiographs were selected. The variables analyzed by ImageJ™ and Nemoceph™ software’s were FP-MP, ANB angle, OPT-SN, CVT-SN and Ad1-Ba. Descriptive and comparative statistical analysis were carried out with IBM SPSS Statistics™ software, subsequently finding intra-examiner agreement. P-values obtained for each of these variables were 0.846 for FP-MP, 0.008 for ANB angle, 0.155 for OPT-SN, 0.415 for CVT-SN, and 0.221 for CVT-SN. Based on these results, we believe that the craniofacial position in the different occlusions could be determined by the fact that the development has not yet been completed.
The relationship between dentistry and posture has been a constant source of interest and research in recent decades1-3. Malocclusion is not only the result of the action of genetic and environmental factors, but also postural ones. Cervical alterations such as fusions and posterior arch deficiencies can be observed in patients with occlusal alterations2 .
However, there are several systematic reviews that demonstrate a lack of reliable scientific information on this relationship, especially in developing patients. This confusion is partly due to the great variety of methodological approaches and errors in studies carried out4-7.
Authors such as Aranitasi et al,2 affirm that nonsyndromic patients with skeletal class II or III have a high prevalence of fusion between cervical vertebrae. According to Lippold et al,8 there are associations between occlusion anomalies and scoliosis in preschool populations. Solow and Sonnesen9 observed a clear association pattern between crowding of more than 2 mm and craniocervical posture in paediatric patients.
For D’Attilio et al,10 children with skeletal class III may have a significantly lower angle of cervical lordosis compared to those of skeletal classes I and II; with a significantly greater extension of the head over the spine in class II malocclusions, when compared with skeletal classes I and III.
According to Gogola et al,11 infants with defective postures have more marked malocclusions than those with correct body posture.
Another aspect to take into account in this area is the importance of the airway. Therefore, when evaluating the nasal pathway and oropharyngeal volumes in children and with different dentofacial skeletal patterns, it was observed that the position of the mandible with respect to the cranial base had an effect on the airway volume12. For Kim et al,13 head posture in children and adolescents is associated with different craniofacial dimensions, thereby determining an aetiological respiratory component in cases with open bite.
Sidlauskiene et al,14 analysed occlusion and general body posture in children, as well as nasopharyngeal pathology, such as deviations in the nasal septum, hypertrophy of adenoids, tonsils and allergic rhinitis. They found a statistically significant relationship between the presence of a kyphotic posture and a reduction in the SNB angle, representing the sagittal position of the jaw; and a statistically significant association between kyphotic posture and nasopharyngeal obstruction.
Rocha et al,3 when evaluating the mode of respiration, occlusion and posture parameters in children and adolescents, observed a lower position of the hyoid bone with respect to the plane of the jaw in some study groups with oral respiration. For Silvestrini et al,15 postural, orthoptic, osteopathic and occlusion variables were often clinically associated in children; therefore, all these disorders seem to require a multidisciplinary medical approach for their treatment.
These aforementioned precedents demonstrate that the relationship between occlusion and posture has been a continuing source of interest for all professionals in the provision of health care over the last decades. According to Perinetti16, this importance lies in the fact that dental malocclusion is very highly prevalent among children; therefore, its potential negative effects on body posture could provide other indications for orthodontic treatments.
The lack of consensus among different investigations and the few studies in developing patients invites us to study the craniocervical position in different occlusions in this population.