Original article
Radiographic diagnosis of impacted maxillary canines: Comparison between two and three dimensions
Introduction: An impacted canine is a very common condition and raises several clinical complications. Early and exact diagnosis is important in order to minimise the risks and subsequent complications. The objective of this study is to analyse the effectiveness of two dimensions in the volumetric diagnosis for impacted maxillary canines, using the lines proposed by Alqerban as a reference.
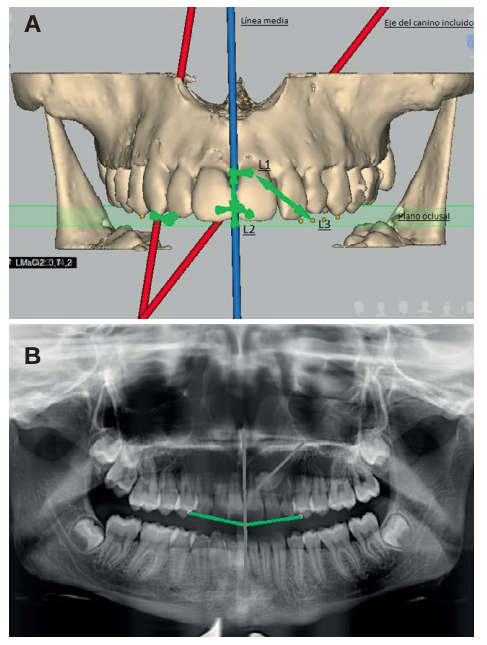
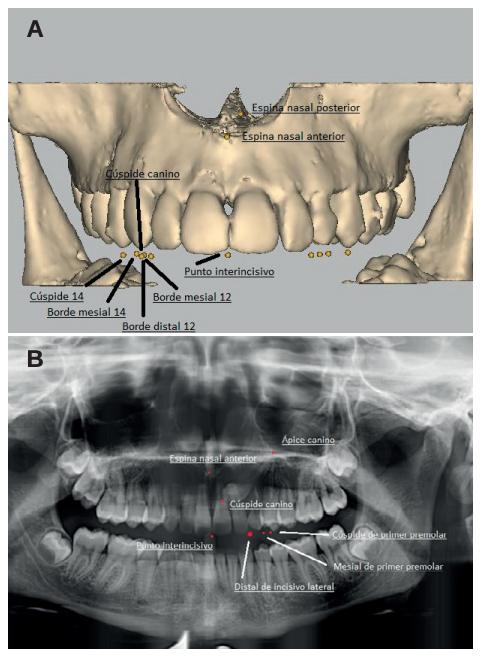
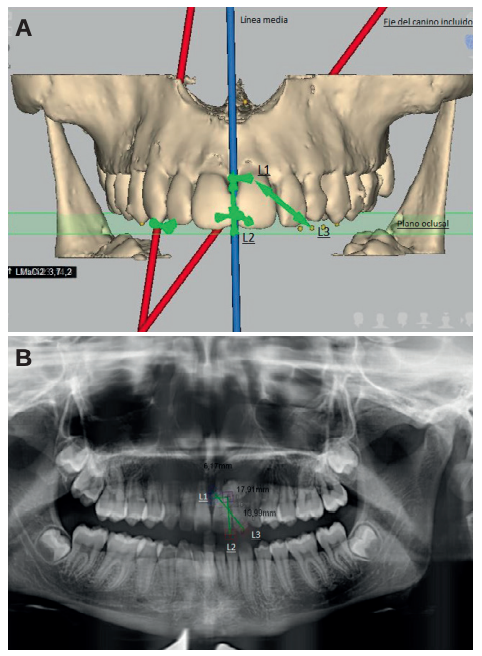
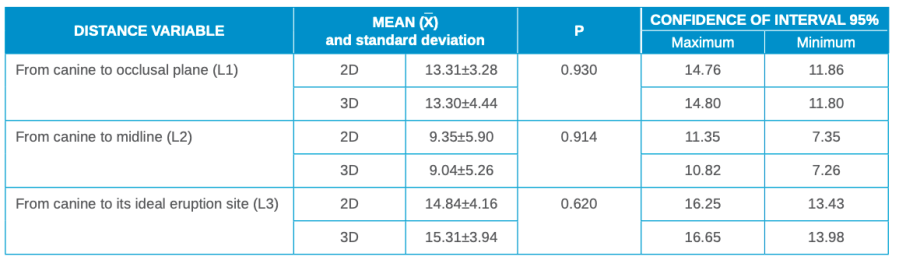
Methods: An orthodontic study of the maxilla using orthopantomography with cone beam computed tomography (CBCT) at the Madrid European University Clinic was performed on 27 patients selected with 36 maxillary impacted canines. Three reference lines were drawn based on the distance from the cusp of the canine to the occlusal plane (L1), to the midline (L2) and to its ideal eruption site (L3), in both the orthopanthomography and the CBCT. As ideal reference values, we selected a control group of 36 erupted maxillary canines.
Results: The results were compared in 2 and 3 dimensions using the Student’s t test, after verifying their normal distribution using the Anderson-Darling contrast test. Statistical significance (p > 0.05) was not obtained for any of the variables studied.
Conclusions: The use of CBCT is vital to ensure good diagnosis of the canine position and its relationship with adjacent structures and thus establish an adequate treatment plan. However, orthopantomography provides sufficient information for initial planning.
Canines are of vital importance in facial and oral aesthetics, as well as in the functionality and development of occlusion. Both Andrews1 with his six keys to occlusion and the latest articles by Clark2 demonstrate the importance of the canine in occlusion. There is no doubt that the canine is one of the pillars in the ideal occlusion scheme proposed by nature. If it is in an aberrant position, it can cause alterations in the entire occlusion system. Due to its anatomy, the maxillary canine guides mandibular movements and supports the forces of occlusion, with a large crown compared to the size of the mandibular tooth itself, and is the tooth with the greatest stability. Its roots are the longest and widest, so these teeth have a firm anchorage in the alveolar bone. Clinically, canines are the teeth that should be lost last. Due to their strategic location in the mouth, they are the cornerstones of the dental arch3 .
The maxillary canine is the permanent tooth with the longest eruption path. It begins forming with a mesial tilt and rapid growth, then slows down as it straightens or even shows a slightly distal diversion.4 This change in speed and inclination corresponds to the contact of the canine with the distal area of the lateral incisor, at approximately 9 years of age. Hence the important role played by the upper lateral incisor in the eruption of the canine. The prevalence and incidence of an impacted maxillary canine is widely reported in the literature. The earliest articles we found in this regard were by Cramer in 19295 and Mead in 19306 . These describe an incidence of 1.4% and 1.57%, respectively, after selecting a sample of American white males. Other authors expand and modify the sample, and obtain prevalences of 0.92% (Dachi7 ), 1.8% (Thilander and Jakobsson8 ), 2.2% (Thilander and Myberg9 ), 3.61% (Aitasa- lo10) and 2.8% (Ericson and Kurol4,11-13).
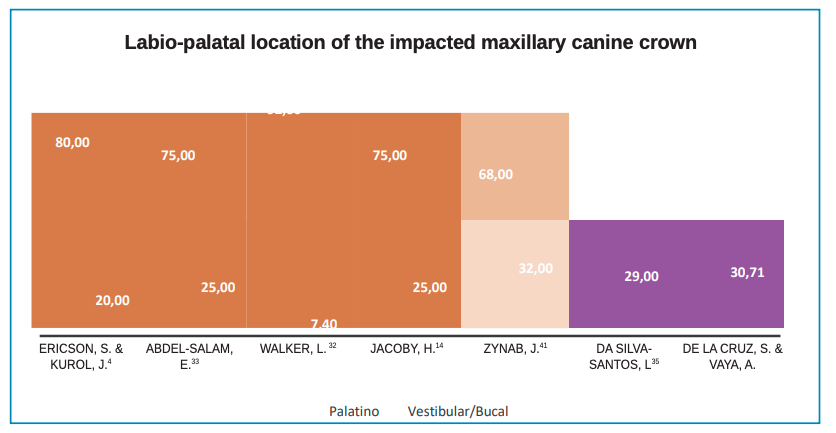
For the interarch position, the classification refers to maxillary canines impacted by the palatal or vestibular. According to this classification14, Jacoby found that 92.31% of patients (a ratio of 12:1) had a palatal impaction, on later expansion of the sample, a ratio of 6.6:1, palatal vs vestibular, was found. Other authors, such as Gaulis and Joho15 obtained a ratio lower than 2:1. The international consensus is for a ratio of 3:1. The current classification, proposed by authors such as Stivaros and Mandall16, reduces the percentage of palatal inclusions to 61%, while vestibular inclusions appear in 5% of patients. For these authors, 34% of canines would be positioned at an intermediate point in the arch. For Rimes et al,17 the proportion of canines impacted palatally is 44%, while those displaced in the vestibular position is 38%. Syrynska18, however, reported 60.3% for palatal canines and 20.6% for vestibular; while 19.2% were in an intermediate position in the alveolus.
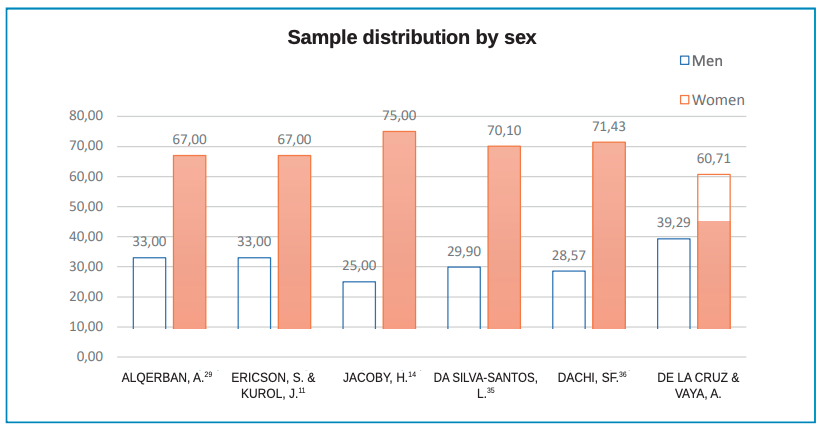
The literature suggests impaction occurs more in women than men. Dachi7 reports 78.57%, Gashi19 77.10% and Bishara20 suggests a ratio of 2:1 for maxillary canine impaction in women over men, which is confirmed by Cooke21.
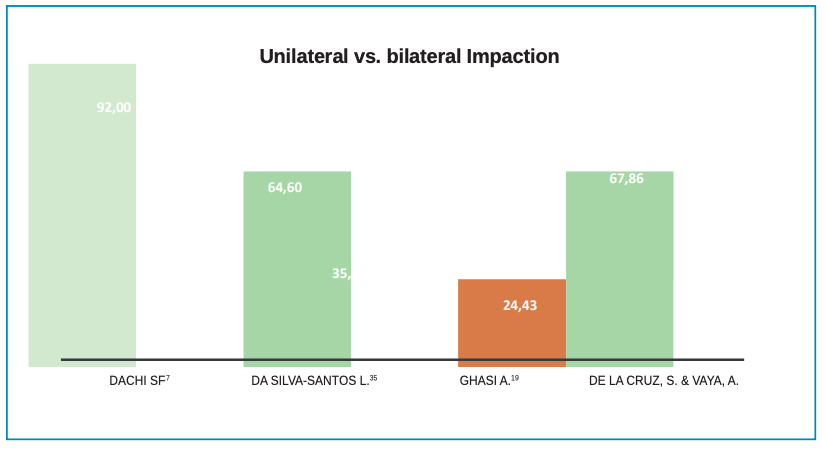
Regarding bilaterality, 8% of patients have a bilateral impaction according to Dachi7 , Bishara20, Manne22 and Yadav23. Shirazi24, however, found no association in gender for unilateral or bilateral impaction in maxillary canines.
Most authors associate palatal inclusion with the Caucasian race, at 5.9%, while vestibular inclusion is associated with Asians, 1.7%25-27. The impaction ratio of Caucasian patients to African or Asian patients is 2:1, according to Peck and Peck28. Etiological factors associated with impacted canines are shown in Table 1.