Caso clínico
¿Es la pulpotomía una alternativa al tratamiento de conductos para los dientes con síntomas de pulpitis irreversible? A propósito de un caso
La pulpotomía total o parcial es una opción terapéutica conservadora para los dientes permanentes con ápice cerrado con signos y síntomas de pulpitis irreversible. Permite preservar los mecanismos de defensa inmune y el potencial regenerativo del tejido pulpar sano remanente, mantiene la integridad estructural del diente y disminuye las complicaciones asociadas al tratamiento de conductos.
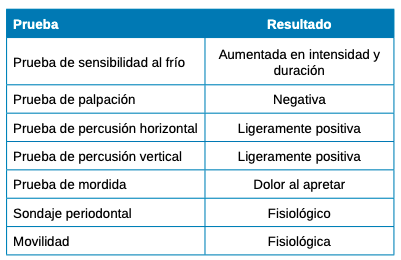
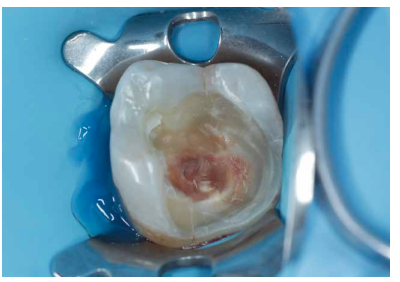
En el presente caso clínico se describe el tratamiento de un 3.7 con diagnóstico de pulpitis irreversible y periodontitis apical sintomática en el que se llevó a cabo una pulpotomía parcial con Biodentine® (Septodont, Sant-Maur-des-Fossés, Francia) durante las prácticas clínicas del Máster de Odontología Restauradora Estética y Endodoncia de la Universidad Rey Juan Carlos. Se presenta el seguimiento a 18 meses.
Complete or partial pulpotomy is a conservative therapeutic option for permanent teeth with closed apex with signs and symptoms of irreversible pulpitis. It preserves the immune defence mechanisms and regenerative potential of the remaining healthy pulp tissue, maintains the structural integrity of the tooth and reduces complications associated with root canal treatment.
This case report describes the treatment of a 3.7 with a diagnosis of irreversible pulpitis and symptomatic apical periodontitis in which a partial pulpotomy was performed with Biodentine® (Septodont, Sant-Maur-des-Fossés, France) during the clinical practice of the Master’s Degree in Aesthetic Restorative Dentistry and Endodontics at the Rey Juan Carlos University. The 18-month follow-up is presented.
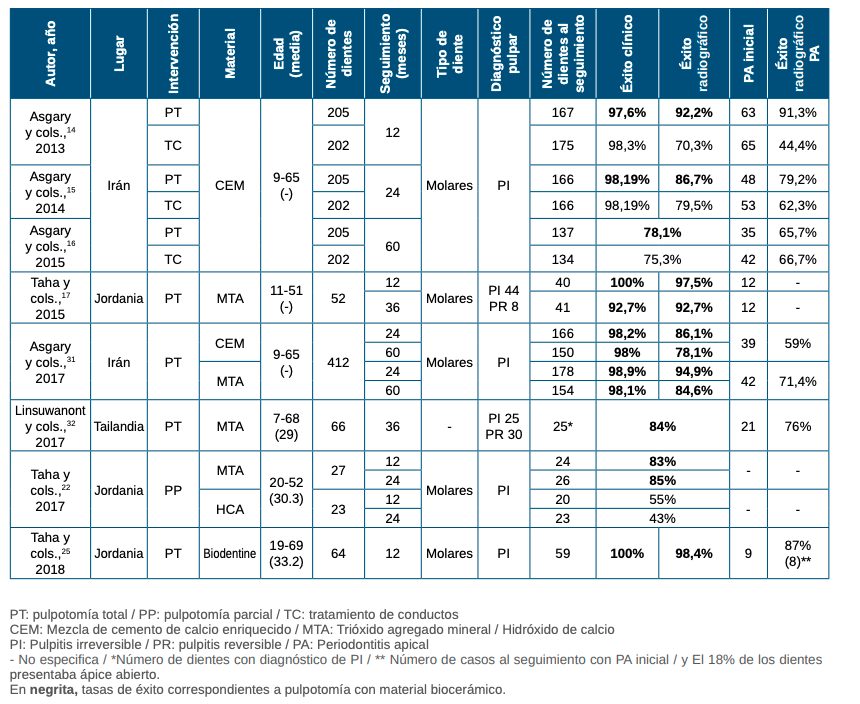
La pulpotomía total se define como la remoción de la porción coronal de la pulpa vital preservando la vitalidad de la porción radicular restante, mientras que la pulpotomía parcial o de Cvek consiste en la remoción de una pequeña porción de la pulpa vital coronal preservando el tejido pulpar remanente coronal y radicular1 . Tradicionalmente, la indicación de la pulpotomía parcial se reducía a dientes permanentes con ápice abierto, y la total era un tratamiento restringido a dentición temporal. Sin embargo, con el desarrollo de los materiales biocerámicos y la mejora en el conocimiento de la biología pulpar y su respuesta ante el proceso carioso, la pulpotomía total o, incluso, la parcial, se han convertido en alternativas terapéuticas definitivas frente al tratamiento de conductos en dientes permanentes con ápice cerrado con signos y síntomas de pulpitis irreversible2 .
Este tratamiento mínimamente invasivo, permite preservar los mecanismos de defensa inmune y el potencial regenerativo del tejido pulpar sano remanente, manteniendo la integridad estructural del diente y disminuyendo las complicaciones asociadas al tratamiento de conductos. También permite reducir costes y posibles molestias a los pacientes3 . Sin embargo, será fundamental para conseguir el éxito a largo plazo considerar una serie de requisitos: una correcta selección del caso, trabajar en condiciones de asepsia, utilizar un biomaterial adecuado y realizar un correcto sellado coronal2 .
El caso clínico expuesto a continuación describe la realización de una pulpotomía parcial con Biodentine® (Septodont, Sant-Maur-des-Fossés, Francia) en un 3.7 que presentaba pulpitis irreversible y periodontitis apical sintomática. Se presenta la revisión a 18 meses.