Revisión bibliográfica
Preservación alveolar con colgajo vs sin colgajo
Introducción: La extracción dentaria desencadena una serie de cambios dimensionales en la altura y anchura de la cresta alveolar que se traducen en la pérdida de tejidos blandos y duros, afectando de forma directa a la calidad de vida de los pacientes. Por ello, se han estudiado diferentes técnicas para la preservación de la cresta alveolar (PCA) tras las extracciones, con el fin de optimizar los resultados funcionales y estéticos de la futura rehabilitación prostodóncica. El objetivo fue evaluar los resultados de la PCA utilizando un enfoque con colgajo en comparación con un enfoque sin colgajo en términos de cambios óseos en anchura y altura.
Material y Métodos: Se realizó una búsqueda bibliográfica en tres bases de datos The National Library of Medicine (MEDLINE/PubMed), Scielo y Cochrane Library. Se incluyeron ensayos clínicos aleatorizados en humanos que compararan la PCA con colgajo y sin colgajo, en los que se analizaran pacientes sanos, mayores de edad, sin hábitos nocivos, en los que era necesaria la exodoncia de un diente mandibular o maxilar.
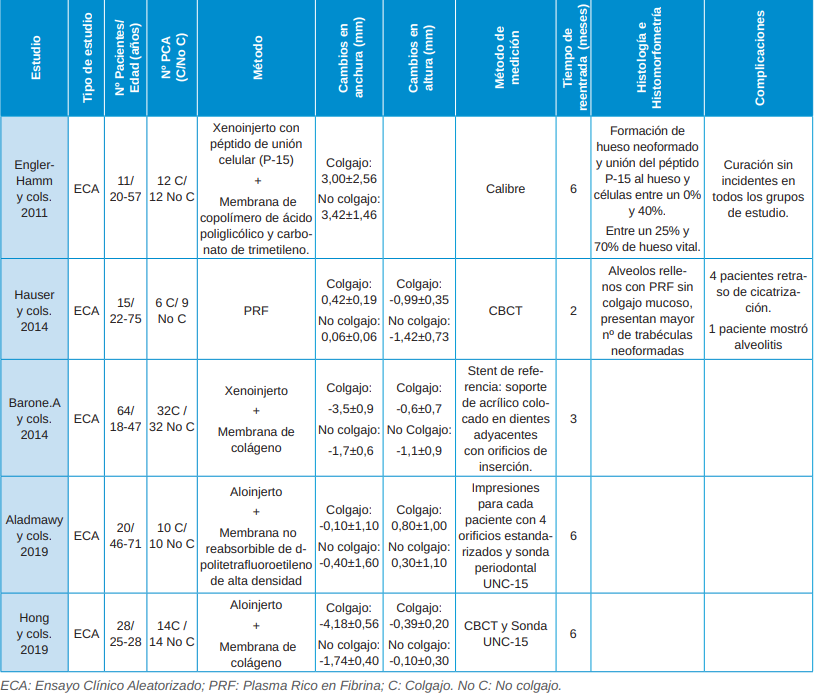
Resultados: Se incluyeron 5 ensayos clínicos de los últimos 15 años en los que se realizó un total de 74 procedimientos quirúrgicos de PCA con colgajo y 77 sin colgajo en 138 pacientes entre 18 y 75 años, cuyo género sólo se describió en 3 estudios. Los cambios óseos en anchura al realizar una PCA con colgajo varían entre –4,18 mm y 3 mm, mientras que al realizar una PCA sin colgajo los cambios son entre 1,74 mm y 3,42 mm. Por otro lado, los cambios óseos en altura al realizar una PCA con colgajo varían entre –0,99 mm y 0,8 mm, mientras que al realizar una PCA sin colgajo los cambios son entre 0,3 mm y 1,42 mm.
Conclusiones: Se produce mayor pérdida en anchura y altura en la PCA cuando se lleva a cabo un colgajo mucoperióstico, aunque son necesarios más ensayos clínicos aleatorizados para poder afirmarlo con mayor rotundidad.
Introduction: Tooth extraction triggers a series of dimensional changes in the height and width of the alveolar ridge, which result in the loss of soft and hard tissues, directly affecting patients’ quality of life. Therefore, different techniques for the preservation of the alveolar ridge (PCA) after extractions have been studied in order to optimize the functional and esthetic results of future prosthodontic rehabilitation. The aim was to evaluate the results of PCA using a flap approach compared to a flapless approach in terms of bone changes in width and height.
Material and Methods: A literature search was performed in three databases The National Library of Medicine (MEDLINE/ PubMed), Scielo and Cochrane Library. Randomized human clinical trials comparing flap and flapless PCA were included in which healthy patients, over the age of majority, without harmful habits, who needed to have a mandibular or maxillary tooth extraction, were analyzed.
Results: A total of 5 clinical trials from the last 15 years were included in which a total of 74 flap and 77 flapless PCA surgical procedures were performed in 138 patients between 18 and 75 years of age and whose gender was only described in 3 studies. Bone changes in width when performing a flapless PCA varied between –4.18 mm and 3 mm, while when performing a flapless PCA the changes were between 1.74 mm and 3.42 mm. On the other hand, bone changes in height when performing a PCA with flap vary between –0.99 mm and 0.8 mm, while when performing a PCA without flap the changes are between 0.3 mm and 1.42 mm.
Conclusions: There is greater loss in width and height in PCA when a mucoperiosteal flap is performed, although more randomized clinical trials are needed to be able to state this more emphatically
Las extracciones dentarias desencadenan una pérdida de hueso alveolar aproximadamente entre el 29-63% en anchura y el 11-22% en altura, estimándose en una reducción media de 3,8 mm de anchura y 1,24 mm de altura durante los primeros seis meses1. Además, se sabe que existen una serie de características anatómicas, fisiológicas y técnicas que influyen en una mayor reabsorción ósea tras la exodoncia, entre las que se encuentran: corticales vestibulares menores a 1 mm, biotipos gingivales finos, exodoncias traumáticas y enfermedades que influyen en el periodo de cicatrización como la diabetes2,3. Se conoce el orden predecible de la reabsorción ósea, siendo la cortical vestibular la que se reabsorbe en primer lugar2,3. Además, hay mayor reabsorción en anchura que en altura4 y el hueso mandibular se reabsorbe más rápido que el maxilar5,6. La atrofia por desuso, la vascularización inadecuada y la respuesta inflamatoria se han implicado como diferentes factores causantes de la reabsorción de la cresta alveolar7.
Se han descrito diferentes procedimientos quirúrgicos para minimizar esta pérdida ósea post-extracción, que van desde las técnicas regenerativas para la conservación del alveolo8-10 hasta la colocación inmediata de implantes11. La preservación de la cresta alveolar (PCA) es un procedimiento encaminado a minimizar los cambios en los tejidos blandos y duros tras la extracción de un diente, con el fin de optimizar los resultados funcionales y estéticos de la futura rehabilitación prostodóncica12,13. Para llevar a cabo la PCA se han utilizado diferentes biomateriales: autólogos, aloinjertos, xenoinjertos e injertos aloplásticos, utilizados con o sin membranas asociadas.
Por otro lado, también se ha descrito el sellado del alveolo con injertos gingivales libres o de tejido conectivo, mediante el uso de materiales biológicamente activos y factores de crecimiento, o una combinación de más de un método14-16. Tras colocar el biomaterial en el alveolo, no se sabe actualmente si se consiguen resultados más favorables al realizar un cierre primario de la herida, en comparación con un cierre por segunda intención, en el que la membrana barrera se deja expuesta. Por tanto, el objetivo de esta revisión narrativa es evaluar los resultados de la PCA utilizando un enfoque con colgajo en comparación con un enfoque sin colgajo en términos de cambios en los tejidos duros. Además, se analizarán los cambios histológicos e histomorfométricos y las complicaciones registradas de cada estudio.