Caso clínico
Vila-Sánchez A, Moreno-López LA. Patología sistémica múltiple en la consulta dental. A propósito de un caso ¿especial?. Cient. Dent. 2021; 18; 5; 321-330
Patología sistémica múltiple en la consulta dental. A propósito de un caso ¿especial?
Resumen
Introducción: La esperanza de vida en España es de las más altas del mundo. Este aumento en la esperanza de vida va unido a una mayor prevalencia de pacientes con pluripatología y polimedicación.
Por lo tanto, la probabilidad de encontrar un paciente con múltiple afectación sistémica y gran carga farmacológica ha aumentado, de tal manera que lo especial se convierte en habitual.
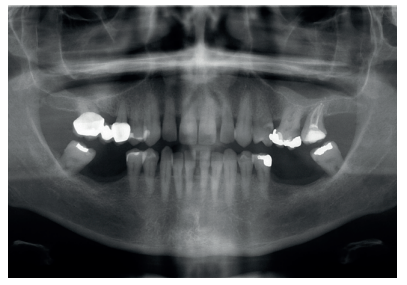
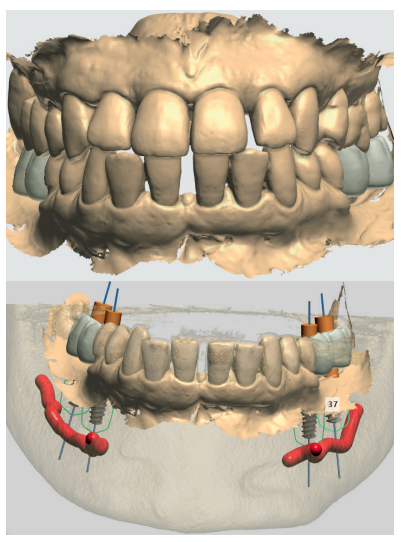
Caso clínico: Se presenta el caso clínico de una paciente con hipertensión, diabetes tipo II, hipotiroidismo, depresión, obesidad y déficit de vitamina D. Se hace una revisión de la actuación del odontólogo en la clínica cuando se presentan pacientes con dichos cuadros y las consideraciones a tener en cuenta con respecto a la prescripción y administración de medicación. El objetivo es presentar recomendaciones de tratamiento a partir de un caso clínico de una paciente con varias afecciones sistémicas en la que se realiza un tratamiento multidisciplinar. Para eso se ha realizado una revisión narrativa que se considera útil para la actividad clínica diaria
Conclusiones: Los pacientes con pluripatologías y con polimedicación no deben suponer un problema en la clínica dental. Sus patologías sistémicas suelen estar interrelacionadas y relacionadas con su patología oral por lo que mejoras esta contribuye a controlar mejor las otras. Deberíamos cuestionarnos a qué nos referimos cuando utilizamos el término “paciente especial”, ¿existe algún paciente que no sea especial?
Abstract
Introduction: Life expectancy in Spain is one of the highest in the world. This increase in life expectancy is linked to a higher prevalence of patients with multiple pathologies and polypharmacy.
Therefore, the probability of finding a patient with multiple systemic involvement and a high drug burden has increased, in such a way that the special becomes common.
Clinical case: The clinical case of a patient with hypertension, type II diabetes, hypothyroidism, depression, obesity and vit D deficiency is presented. A review is made of the performance of the dentist in the clinic when patients with these conditions appear and the considerations to take into account with respect to the prescription and administration of medication. The objective is to present treatment recommendations based on a clinical case of a patient with several systemic conditions in which a multidisciplinary treatment is carried out. For this, a narrative review has been carried out that is considered useful for daily clinical activity.
Conclusions: patients with multiple pathologies and polymedication should not pose a problem in the dental clinic. Their systemic pathologies are usually interrelated and related to their oral pathology, so improvements in this one contribute to better control the others. We should ask ourselves what we mean when we use the term “special patient”, is there a patient who is not special?
Este artículo está exclusivamente disponible para su descarga en PDF. | 03/24/2024
Palabras clave
Ansiedad, Déficit de vitamina D, Diabetes tipo II, Hipertensión arterial, Hipotensión, Interacciones farmacológicas, Obesidad
Introducción
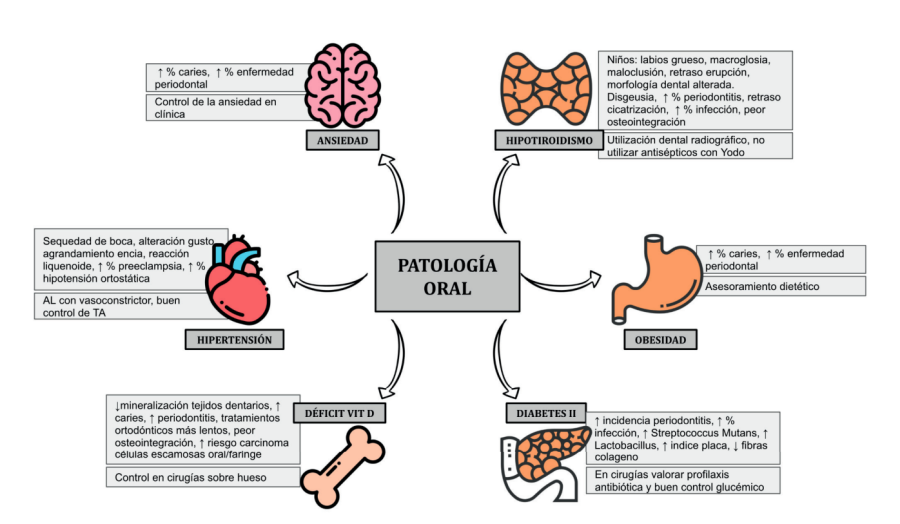
El paciente médicamente comprometido y con presencia de varias comorbilidades en la actualidad es una situación cada vez más frecuente. Entre las patologías frecuentes que padecen los pacientes que pueden acudir a una consulta dental están la diabetes, la hipertensión, el hipotiroidismo, la ansiedad, la obesidad y déficits nutricionales como el de vitamina D1 .
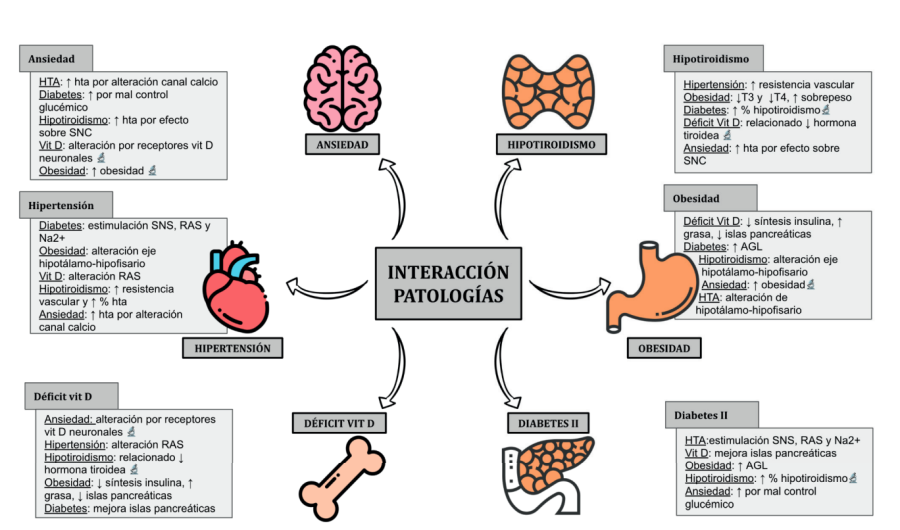
La mayoría de estas condiciones son crónicas y necesitan un tratamiento farmacológico permanente. Además, se suelen encontrar de manera conjunta y el control de una de ellas influye en el control del resto de igual manera que el control de la enfermedad general influye en la salud oral y viceversa2 .
Como parte de nuestra asistencia sanitaria está el investigar la patología y la medicación que presentan nuestros pacientes en la clínica para conocer las posibles interacciones con el desarrollo de nuestra actividad odontológica, como una actividad sanitaria más. Por ello es imprescindible una formación del odontólogo en patología y farmacología general.
Bibliografía
Rivas Costa G, Domínguez Berjón MF, Astray Mochales J, Gènova Maleras R, Rodríguez Laso A, Esteban Vasallo MD. Características epidemiológicas de la pluripatología y su influencia en la utilización de servicios sanitarios a partir de una encuesta de salud. Madrid, 2007. Rev Esp Salud Publica 2009;83(6):835- 846.
Tavares M, Lindefjeld Calabi KA, San Martin L. Systemic diseases and oral health. Dental Clinics of North America 2014;58:797-814.
Bescós E, Crespo A, Arias C, Chaparro M. Hipertensión arterial [Internet] Málaga: Hospital Clínico Universitario Virgen de la Victoria. 2015. Disponible en: http:// www.medynet.com/usuarios/jraguilar/ Manual%20de%20urgencias%20y%20 Emergencias/htaurg.pdf [Consultado y citado junio 2021]
Southerland JH, Gill DG, Gangula PR, Halpern LR, Cardona CY, Mouton ChP Dental management in patients with hypertension: challenges and solutions. Clin Cosmet Invest Dent 2016;8:111.
Ministerio de Sanidad. Gobierno de España. Disponible en: https://www. mscbs.gob.es/ ciudadanos/enfLesiones/ enfNoTransmisibles/diabetes/diabetes. htm. [Consultado y citado junio 2021].
Fundación de la Sociedad Española de Diabetes: https://fundacion.sediabetes. org/. [Consultado y citado junio 2021].
Papatheodorou K, Banach M, Bekiari E, Rizzo M, Edmonds M. Complications of Diabetes 2017. J Diabetes Res 2018: Article ID 3086167.
Taylor GW, Borgnakke WS. Periodontal disease: associations with diabetes, glycemic control and complications. Oral Dis 2008;14:191-203.
Daniel R, Gokulanathan S, Shanmugasundaram N, Lakshmigandhan M, Kavin T. Diabetes and periodontal disease. J Pharm Bioallied Sci 2012; Suppl 2:S280-2.
Venza I, Visalli M, Cucinotta M, D Grazia G, Teti D, Venza M. Proinflammatory gene expression at chronic periodontitis and peri‐implantitis sites in patients with or without type 2 diabetes. J Periodont 2010;81:99-108.
Hintao J, Teanpaisan R, Chongsuvivatwong V, Dahlen G, Rattarasarn C. Root surface and coronal caries in adults with type 2 diabetes mellitus. Com Dent Oral Epidemiol 2007;35:302-309.
Maldonado C. Prevalencia de disfunción tiroidea en la población española. Implicación del hierro en la fisiología tiroidea. Tesis Doctoral. Universidad de Málaga. Facultad de Medicina; 2017.
Sociedad Española Endocrinología y Nutrición. Disponible en: https:// www. seen.es/portal. [Consultado y citado junio 2021].
Chandna S, Bathla M. Oral manifestations of thyroid disorders and its management. Indian J Endocrinol Metab 2011; 15(suppl2):s113.
Hwang D, Wang HL. Medical contraindications to implant therapy: Part II: Relative contraindications. Implant Dent 2007;16: 13-23.
Attard N, Zarb GA. A study of dental implants in medically treated hypothyroid patients. Clin Implant Dent Relat Res 2002;4(4):220-231.
Levine R. Obesity and oral disease–a challenge for dentistry. Br Dent J 2012;213:453-456.
Represa González JC. Estado de salud bucodental en obesos mórbidos. Tesis Doctoral. Universidad Complutense de Madrid. Facultad de Odontología; 2005.
Sociedad Española para el estudio de la ansiedad y el estrés. Disponible en: https://webs.ucm.es/info/seas/faq/ ansiedad.htm. [Consultado y citado junio 2021]
Mohammadi T, Sabouri A, Sabouri S, Najafipour H. Anxiety, depression, and oral health: A population-based study in Southeast of Iran. J Dent Res 2019; 16(3):139.
Jetter A, Egli A, Dawson-Hughes B, y cols. Pharmacokinetics of oral vitamin D3 and calcifediol. Bone 2014; 59:14-19.
Quesada JM, Bouillon R. Is calcifediol better than cholecalciferol for vitamin D supplementation? Osteoporosis Int 2018;29:1697-1711.
Botelho J, Machado V, Proença L, Delgado AS, Mendes JJ. Vitamin D deficiency and oral health: A comprehensive review. Nutrients 2020;12:1471.
Nastri L, Moretti A, Migliaco S, y cols. Do Dietary Supplements and Nutraceuticals Have Effects on Dental Implant Osseointegration? A Scoping Review. Nutrients 2020;12:268.
Instituto Nacional de Estadística. Defunciones según causa de muerte. año 2020. Disponible en:https://www.ine. es/dyngs/INEbase/es/operacion.htm? c=Estadistica_C&cid=1254736176780& menu=ultiDatos&idp=1254735573175. [Consultado y citado junio 2021].
American Diabetes Association. Hypertension management in adults with diabetes. Diabetes care 2004;27(suppl 1): s65-s67.
Verma S. Hussain ME. Obesity and diabetes: an update. Diabetes Metab Syndr Clin Res Rev 2017;11:73-79.
Mathieu C, Gysemans C, Guilietti A, Bouillon R. Vitamin D and diabetes. Diabetologia 2005;48:1247-1257.
Joffe B, Distiller LA. Diabetes mellitus and hypothyroidism: strange bedfellows or mutual companions? World J Diabetes 2014;5:901.
Fuentes LB, Haydeé G, Orellano GO, Trujillo L. Hypothyroidism as a Potential Risk Factor in Hypertensive Patients. Int J Sci 2013;2:22-27.
Verma A, Jayaraman M, Kumar HK, Modi KD. Hypothyroidism and obesity. Saudi Med J 2008;29:1135-1138.
Sanyal D, Raychaudhuri M. Hypothyroidism and obesity: An intriguing link. Indian J Endocrinol Metab 2016;20:554.
Mackawy AMH, Al-AyedL BM, AlRashidi BM. Vitamin D deficiency and its association with thyroid disease. Int J Health Sci 2013;7:267.
Muscogiuri G, Tirabassi G, Bizzaro G, y cols. Vitamin D and thyroid disease: to D or not to D? Eur J Clin Nutr 2015;69: 291–296.
Pilz S, Tomaschitz A, Ritz E, Pieber TR. Vitamin D status and arterial hypertension: a systematic review. Nat Rev Cardiol 2009;6(10):621-630.
Kunutsor SK, Apekey TA, Steur M. Vitamin D and risk of future hypertension: meta-analysis of 283,537 participants. Eur J Epidemiol 2013;28(3):205-21.
Sevavalle G, Grassi G. Obesity and hypertension. Pharmacol Res Commun 2017; 122:1-7.
Collins MM, Corcoran P, Perry IJ. Anxiety and depression symptoms in patients with diabetes. Diabetic Med 2009;26:153-161.
Grigsby AB, Andersen RJ, Freedland KE, Clouse RE, Lustman PJ. Prevalence of anxiety in adults with diabetes: a systematic review. J Psychosomat Res 2002;53:1053-60.
Tunkay T, Musabak I, Gok D, Kutlu M. The relationship between anxiety, coping strategies and characteristics of patients with diabetes. Health Qual Life Outcomes 2008;6:1-9.
Graham N, Smith DJ. Comorbidity of depression and anxiety disorders in patients with hypertension. J Hypertens 2016;34:397-398.
Fischer S, Ehlert U. Hypothalamicpituitary-thyroid (HPT) axis functioning in anxiety disorders. A systematic review. Depress Anxiety 2018;35:98-110.
Armstrong DJ, Meenagh GK, Bickle I, H Lee AS, Curran ES, Finch MB. Vitamin D deficiency is associated with anxiety and depression in fibromyalgia. Clin Rheumatol 2007;26:551-554.
Jorm AF, Korten AE, Christensen H, Jacomb PA, Rodgers B, Parslow RA. Association of obesity with anxiety, depression, and emotional well‐being: a community survey. Aust N Z Publ Health 2003;27:434-440.