Caso clínico
Comportamiento clínico, radiográfico e histomorfométrico del diente autólogo como biomaterial en elevación de seno maxilar de acceso lateral. Caso clínico con seis meses de seguimiento post-carga protésica
Introducción: la pérdida ósea tras las extracciones puede requerir en el maxilar posterior la realización de una elevación de seno para la correcta colocación de implantes. El hueso autólogo se considera el gold estándar, pero tiene una alta tasa de reabsorción y morbilidad, haciendo que haya otras alternativas como el diente autólogo, con buenos resultados en procedimientos regenerativos. Este caso clínico evalúa a nivel clínico, radiográfico e histomorfométrico el empleo del diente autólogo en elevación de seno maxilar y el comportamiento de dos implantes colocados de manera diferida.
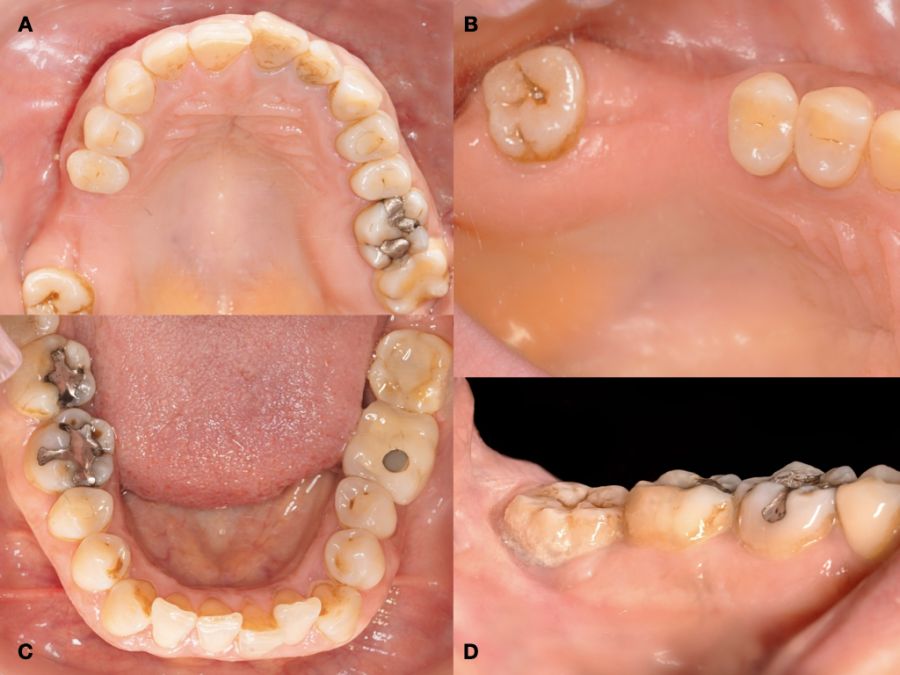
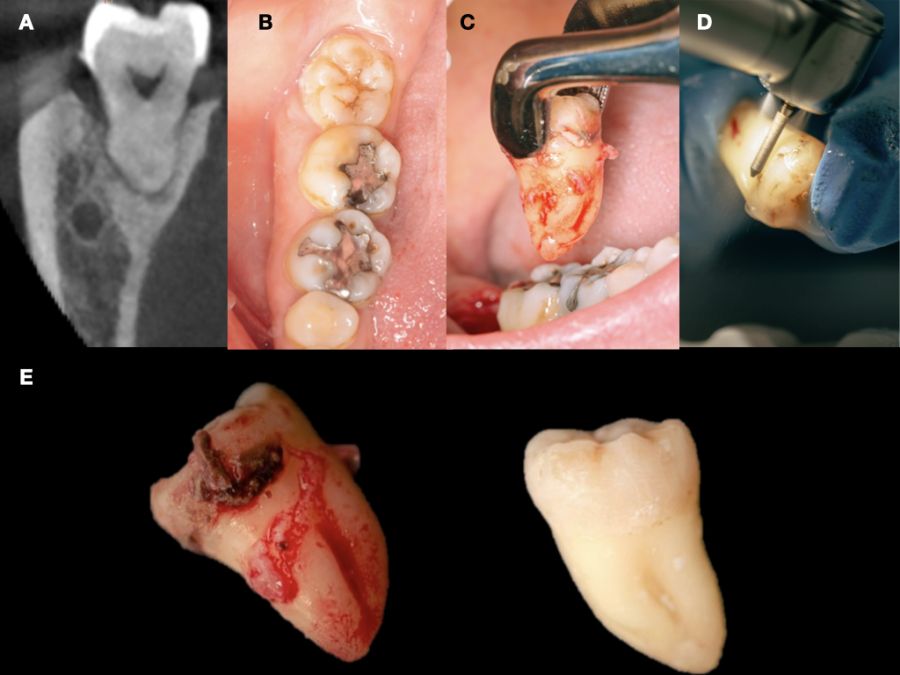
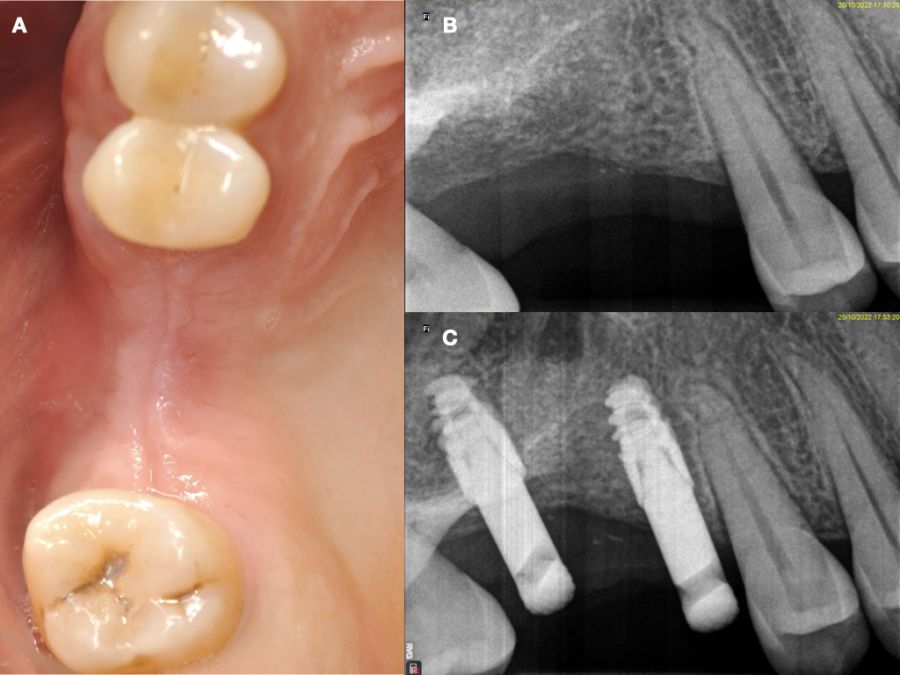
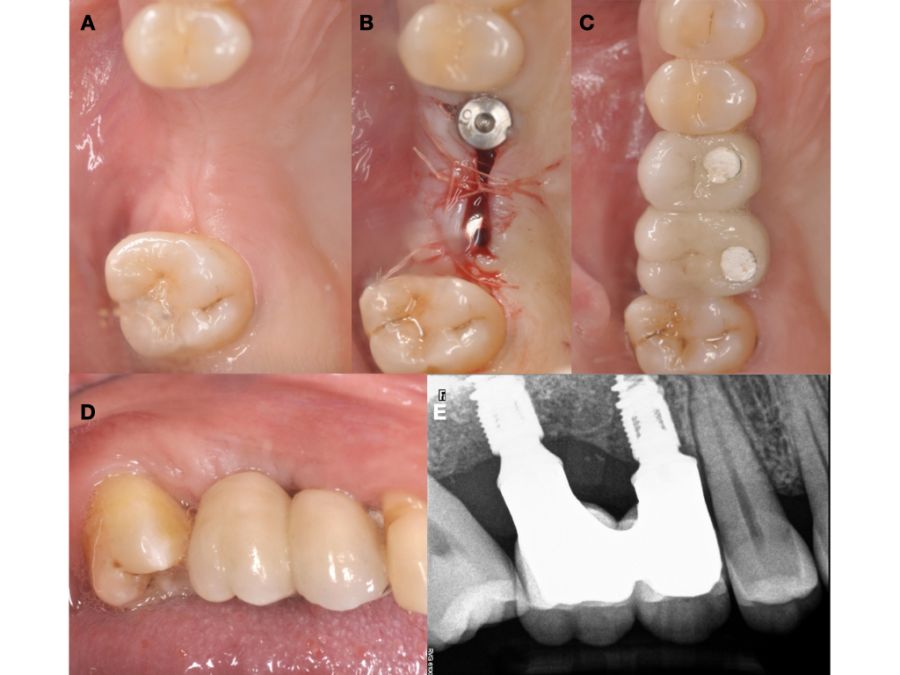
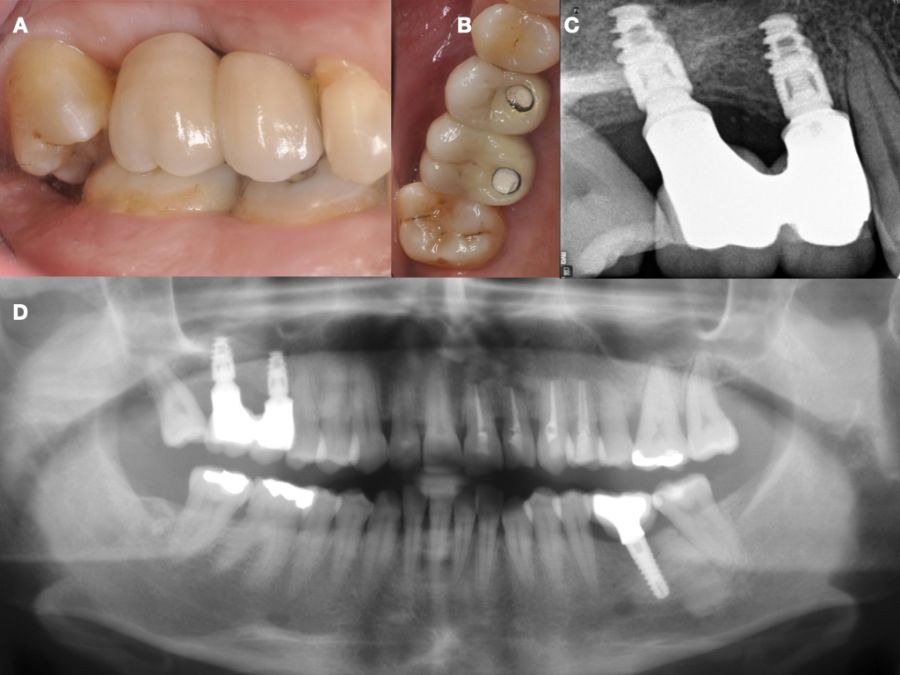
Caso clínico: se presenta el caso de una mujer de 48 años, que acudió a consulta para reponer el sector posterior derecho. Se realizó la exodoncia del 4.8 como diente donante para utilizarlo como biomaterial en una elevación de seno de acceso lateral, colocando dos implantes seis meses tras la intervención, y evaluándolos seis meses tras su carga protésica.
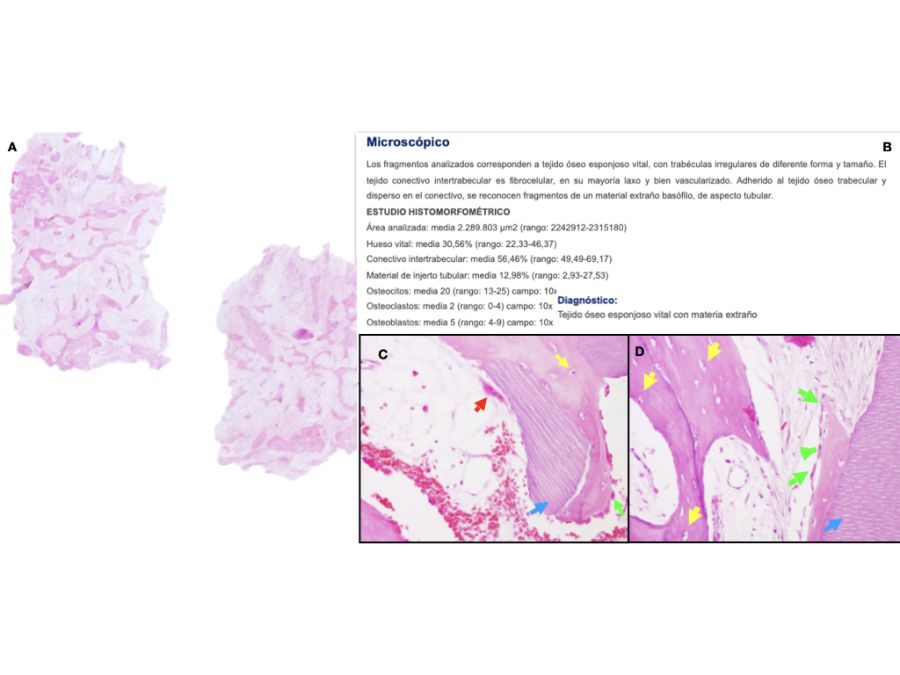
Discusión: el diente autólogo en el presente caso clínico presentó un 30,56% de hueso neoformado tras seis meses de espera, con mejores resultados que al emplear aloinjertos y xenoinjertos. Además, diferentes aspectos culturales y étnicos respaldan la aceptación del diente autólogo por parte de los pacientes, aunque se necesitan más estudios a largo plazo para evaluar la estabilidad de este tipo de injerto en elevación de seno maxilar.
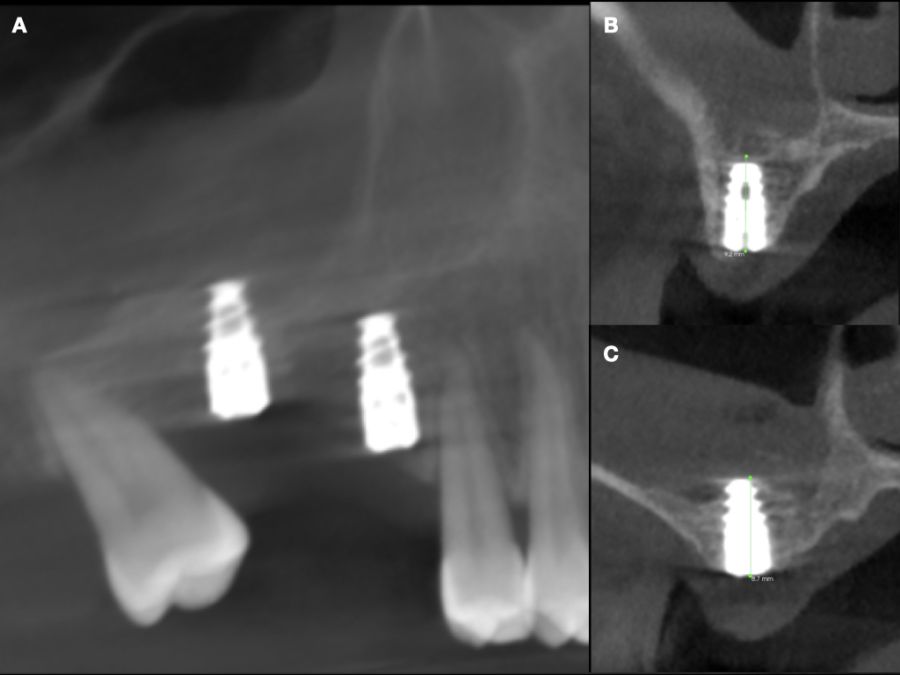
Conclusiones: el diente autólogo en la elevación de seno ofrece biocompatibilidad, baja incidencia de complicaciones y buena aceptación por parte del paciente, con un buen comportamiento clínico y radiográfico de los implantes, a pesar del poco tiempo transcurrido en este caso tras la carga.
Clinical, radiographic and histomorphometric behaviour of the autologous tooth as a biomaterial in lateral access maxillary sinus elevation. Case report with six months of post-prosthetic loading follow-up
Introduction: bone loss after extractions may require a sinus elevation to be performed in the posterior maxilla for the correct placement of implants. Autologous bone is considered the gold standard, but has a high rate of resorption and morbidity, leading to other alternatives such as autologous tooth, with good results in regenerative procedures. This case report evaluates at the clinical, radiographic and histomorphometric level the use of the autologous tooth in maxillary sinus elevation and the behaviour of two implants placed in a delayed manner.
Case report: the case is presented of a 48-year-old woman who came for consultation to replace the right posterior sector. The extraction of 4.8 as a donor tooth was performed to use it as a biomaterial in a lateral access sinus elevation, placing two implants six months after the intervention, and evaluating them six months after their prosthetic loading.
Discussion: the autologous tooth in this case report showed 30.56% of newly formed bone following a six-month wait, with better results than when allografts and xenografts were used. In addition, different cultural and ethnic aspects support the acceptance of the autologous tooth by patients. However, more long-term studies are needed to evaluate the stability of this type of graft in maxillary sinus elevation.
Conclusions: the autologous tooth in the sinus elevation offers biocompatibility, low incidence of complications and good patient acceptance, with good clinical and radiographic behaviour of the implants, despite the short time elapsed in this case after loading.
Keywords: Autologous tooth; Lateral sinus elevation; Autologous dentin.
Tres meses tras una extracción dental, se produce una pérdida del 50% de las dimensiones óseas iniciales del alveolo, cobrando especial importancia en la región posterior del maxilar. En esta región anatómica, la pérdida de los dientes antrales produce una neumatización tridimensional del seno maxilar, pudiendo alcanzar la cresta alveolar y la región anterior, la zona tuberositaria y el hueso cigomático. Este doble proceso de neumatización y remodelación ósea reduce la disponibilidad ósea en sentido horizontal y vertical, pudiendo comprometer el tratamiento con implantes y su estabilidad a largo plazo1-6.
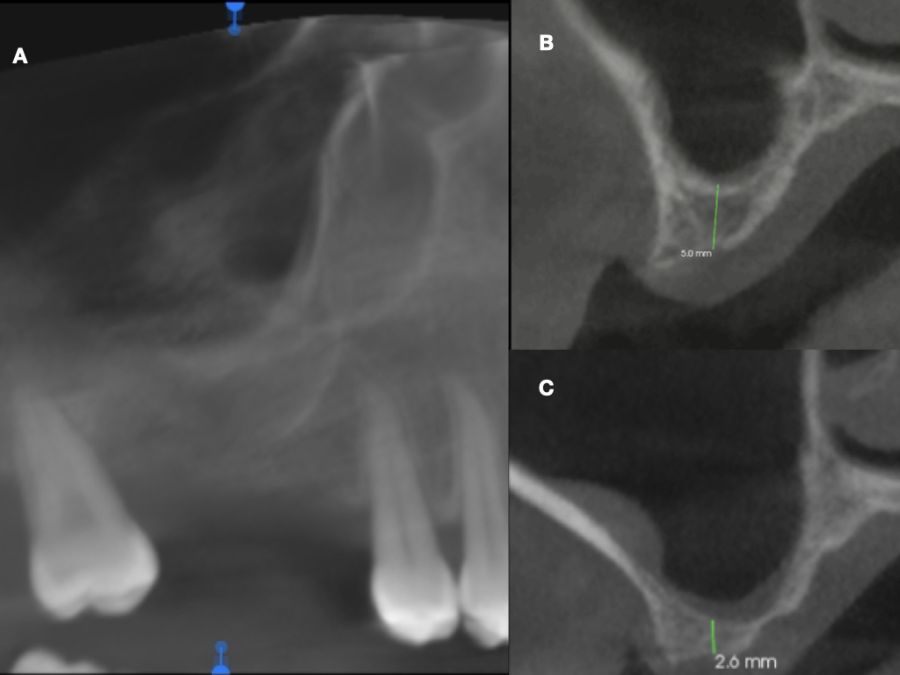
En estos casos, la técnica más predecible para la reconstrucción ósea es la elevación de seno maxilar, que permite una correcta colocación de implantes y su posterior restauración implantosoportada, mejorando la cantidad y calidad ósea del lecho implantado. Entre las técnicas de elevación del seno maxilar, la técnica de acceso lateral está indicada cuando la altura ósea vertical es ≤ 4 mm, colocando los implantes de manera diferida, mientras que con una altura ≥ 5 mm, se recomienda la técnica de elevación de seno transcrestal e implantes más cortos, o técnica abierta con implantes simultáneos de mayor longitud7,8.
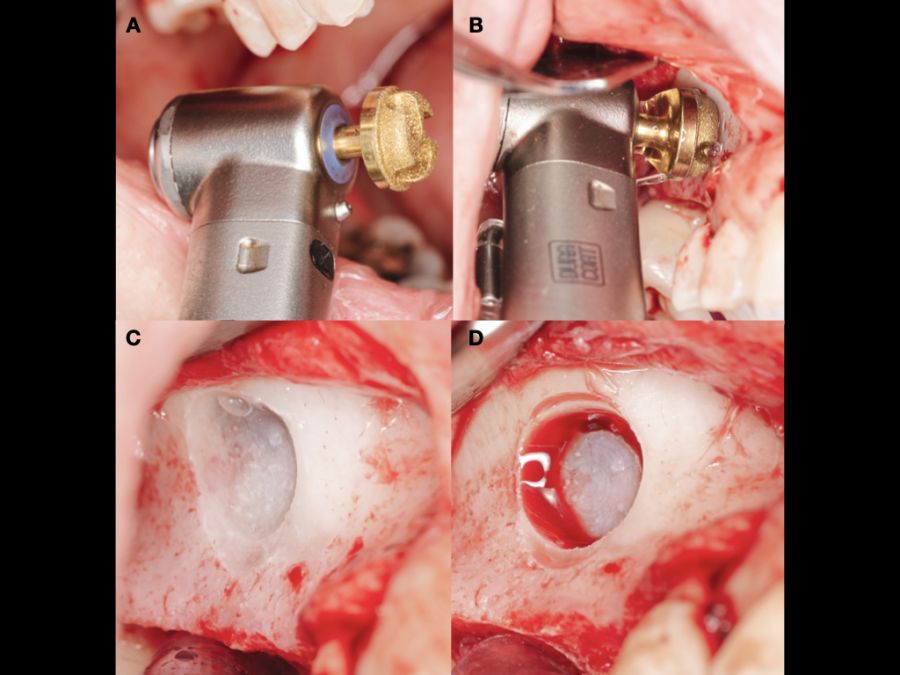
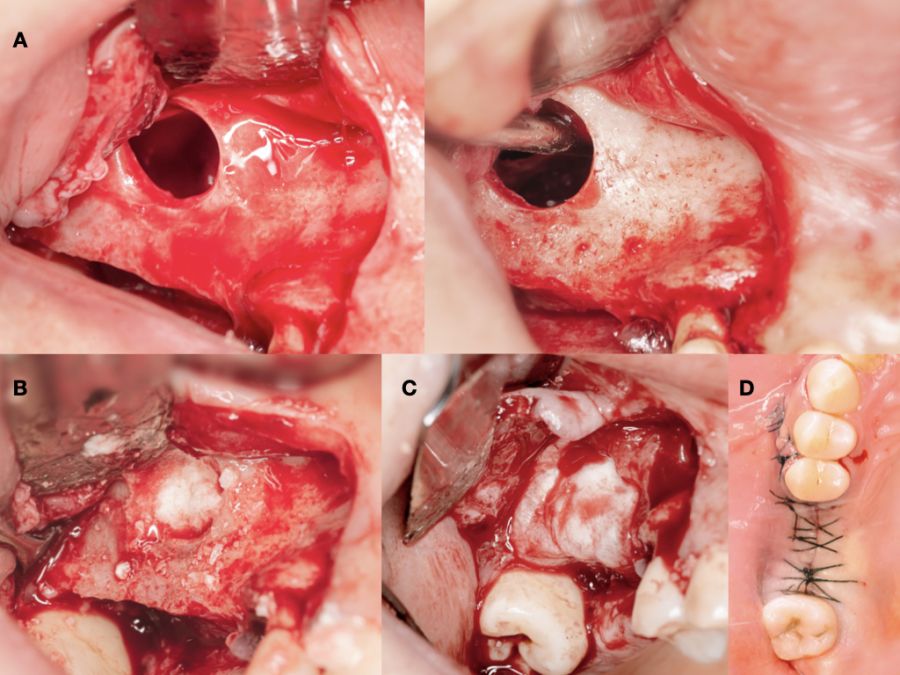
La elevación de seno de acceso lateral, también denominada técnica abierta, es una técnica bien documentada, habiendo sido descrita por Tatum9 en 1976 y publicada posteriormente por Boyne y James10 en 1980. Consiste en la realización de un colgajo a espesor total, para poder acceder a la cara anteroexterna del seno maxilar, y mediante osteotomía realizar una ventana en la cortical vestibular, exponiendo la membrana de Schneider. Una vez expuesta esta membrana, será despegada cuidadosamente y se elevará hasta tener una posición horizontal para formar el nuevo suelo del seno, colocándose posteriormente un biomaterial de relleno. Se puede colocar una membrana reabsorbible o no antes de suturar, para evitar el desplazamiento del injerto y la colonización del interior del seno por el periostio procedente del colgajo11,12.
Entre los biomateriales empleados en esta técnica, el hueso autólogo es actualmente considerado como gold standard debido a que proporciona un buen andamiaje para la osteoconducción, contiene factores de crecimiento para favorecer la osteoinducción y células osteocompetentes para permitir los procesos de osteogénesis, aunque ciertos inconvenientes como la morbilidad de la zona donante, su limitada disponibilidad y su alta tasa de reabsorción, pueden condicionar su uso13,14.
Por estos motivos se han empleado diferentes sustitutos óseos (aloinjertos, xenoinjertos y materiales aloplásticos). La mayoría de estos biomateriales solo presentan propiedades osteoconductoras y tiempos de reabsorción muy variables, que van desde los muy cortos (derivados del ácido poliglicólico y poliláctico) a los muy largos (hidroxiapatitas), mientras que otros pueden presentar reacciones inmunes (aloinjertos). Debido a estas desventajas, se han incrementado en los últimos años los estudios sobre el comportamiento del diente en diferentes procedimientos regenerativos, por su similitud con el hueso humano15,16.
Kim y cols.17describieron las propiedades osteoinductivas y osteoconductoras del diente, así como una menor morbilidad y mayor aceptación por parte del paciente, habiéndose demostrado su buen comportamiento clínico y radiográfico en procedimientos de elevación de seno maxilar, regeneración ósea guiada y preservación alveolar18.
El objetivo del presente caso clínico es evaluar clínica, radiográfica e histomorfométricamente el uso del diente autólogo como biomaterial en elevación de seno maxilar, así como el comportamiento clínico y radiográfico de dos implantes colocados de manera diferida a la elevación de seno, y su evolución seis meses tras la carga protésica de los mismos.