Original article
Relationship between the socioeconomic status and the chronology and eruption sequence of permanent dentition
Objective: Relate the eruption process in permanent dentition with the socioeconomic status.
Methods: An epidemiologic, descriptive and cross-sectional study was carried out in the Spanish population, participating 725 children between 4 and 14 years of age, the selection was opportunistic recording in a database the socioeconomic status of the progenitors, the chronology and emergence sequence of each of the permanent teeth.
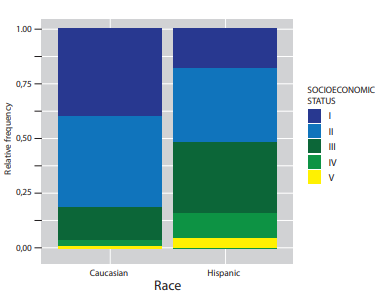
Results: Regarding the socioeconomic status, 38.62% were Level I, 40.83% Level II, 15.86% Level III, 4.14% Level IV and 0.55% Level V. The first tooth to appear in the maxilla was the first molar (74.34-76.41%), while in the mandible it was the central incisor (78.9-82.76%) with statistically significant differences (p-χ2 <0,001).
Conclusions: TThe medical care and nutrition of the patients will depend on the socioeconomic status, but at the dental level there were no statistically significant differences regarding the chronology and eruption sequence
The eruption is a physiological and dynamic process that starts with the formation of the tooth germ, which moves from its crypt in the bone until it emerges in the oral cavity and occludes with its antagonist1-3. This process begins around the age of 6, when the first permanent molar erupts, going from an exclusively temporary to mixed dentition, ending around the age of 12 when the permanent second molar emerge4.
Among the systemic and local factors that can alter both the chronology and the eruption sequence of permanent dentition, are:4.5 sex, age, origin, genetics, bone-dental discrepancy, premature loss of temporary teeth, skeletal development, socioeconomic status and environmental factors5-9. Because of all these factors, establishing a specific age for the emergence is complex. However, it is possible to establish age ranges or averages for the eruption, in order to have a guide for the diagnosis and treatment in paediatric dentistry and orthodontics10.
As for the emergence sequence, it seems that it is a key element for the correct tooth eruption. We consider this as the place occupied by the tooth in the arch11. Moron et al.1 consider the sequence norm stricter than that of the chronology while San Miguel Penton et al. state that, even if the emergence order does not follow the norm, it may be favourable11. The most propitious sequence at the maxillary level is: 6-1-2-4-5-3-7 and in the mandible: 1-6-2-3-4-5-712.
In Spain, the chronology and sequence studies in permanent dentition are scarce, and the last record corresponds to 2013, hence the interest in collecting updated data12. In addition, one of the least studied influencing factors is the socioeconomic status, closely related to the individual nutritional level and the growth and development of oral tissues, especially dental13.
Domingo et al. determined how the lower social classes would have poorer health and less opportunity to highquality health care, worse nutrition, and less physical activity and delayed tooth eruption14.
Based on this, the main objective was to investigate and relate the chronology and sequence of tooth eruption with socioeconomic status.
A cross-sectional descriptive epidemiological study was carried out between November 2020 and September 2021. 733 children from the Community of Madrid (Spain) between 4 and 14 years of age participated.
The population was randomly selected, all went to the Dental Clinic of the European University of Madrid and two private clinics. To determine the sample power, a calculation was made with a standard deviation of 0.5 years, taking into account the age and gender ranges; the minimum number of participants was 620.
The study was carried out in accordance with the Declaration of Helsinki and with the prior approval by the Research Committee of the European University of Madrid and the Ethics Committee of the Community of Madrid of the Medicines Research. At the beginning, parents or legal guardians were informed of the procedure and signed an informed consent for both the study and for the preventive measures due to the Covid-19 pandemic.
The children included enjoyed a good general health. 8 patients were excluded due to dental agenesis, supernumerary teeth and systemic diseases.
A first dental examination was carried out by two researchers. Previously, the patient’s clinical history was reviewed, recording data regarding the date of the visit, age in years and months, origin, sex and socioeconomic status. It was determined as shown below14:
- Directors of public administration and of companies with 10 or more employees. Professions associated with second or third cycle university degrees.
- Managers of companies with less than 10 employees. Professions associated with a first university cycle. Support technicians and professionals. Artists and athletes.
- Administrative and professional staff to support administrative and financial management. Personal services and security workers. Self-employed. Manual work supervisors.
- Skilled and semi-skilled manual workers.
- Unskilled workers.
The researchers recorded the emerged teeth and their sequence under a light source of the dental chair and an intraoral mirror. A tooth was considered to have erupted when any part of its crown had pierced the gingival mucosa according to the criteria established by Carr et al.15 Third molars were excluded from the study. The sequence was recorded according to the eruption of each piece. In those participants with complete permanent dentition, the most common eruption sequence according to the literature was taken into account12.
One week after the first examination, 20% of the sample was re-examined by both researchers. First, the principal investigator performed the examination again and recorded both the sequence and the erupted teeth at that time. Then the second investigator carried out the same procedure recording everything in two different Excel sheets (Microsoft Corp., Redmond, WA, USA). It was considered that one tooth would have erupted when any part of its crown was seen through the gingival mucosa. Intra-observer and interobserver concordance tests were carried out with a kappa value always above 0.95. It was observed that the concordance was almost perfect, being perfect for several of the teeth. professionals. Artists and athletes.
Regarding the quantitative variables, the descriptive statistic was carried out by numerical summaries, and the qualitative with frequency and contingency tables. Subsequently, the chi-square test and Fisher’s exact test were applied.
For the measurement of a factor using logistic regression feedback models, the Wald test, the ROC curve and AUC (Area under the ROC Curve) were applied. The t-test and Wilcoxon test were used for the comparison of two samples, the Welch t-test was required in cases that did not assume the sample’s normalcy.
The homoscedasticity of the sample was studied by the Levene test and a normality was found in those samples large enough according to the central limit theorem.
To compare the averages of two groups, different tests were used according to the homoscedasticity; if this was low, we used the Kruskal-Wallis test, if it was average we used the Welch’s ANOVA test and if it was high the ANOVA test.
The relationship between the numerical variables was carried out using the coefficient and the Spearman correlation test. The results were considered significant for p values below 0.05.
To perform the analysis the statistical software R (version 4.1.1) was used using the RStudio environment (RStudio Inc., Boston, MA, USA).
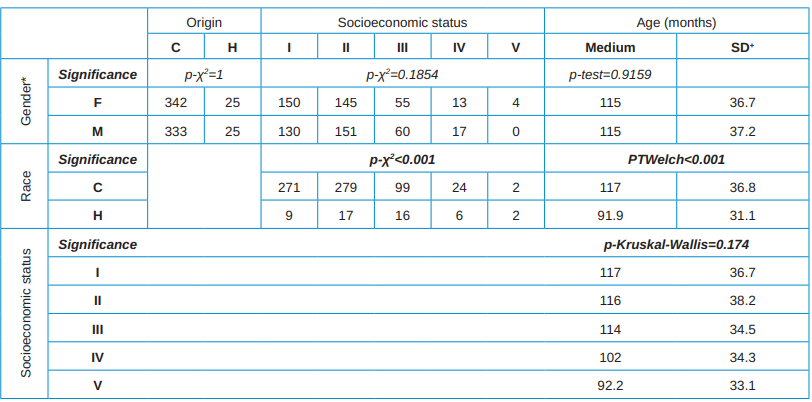
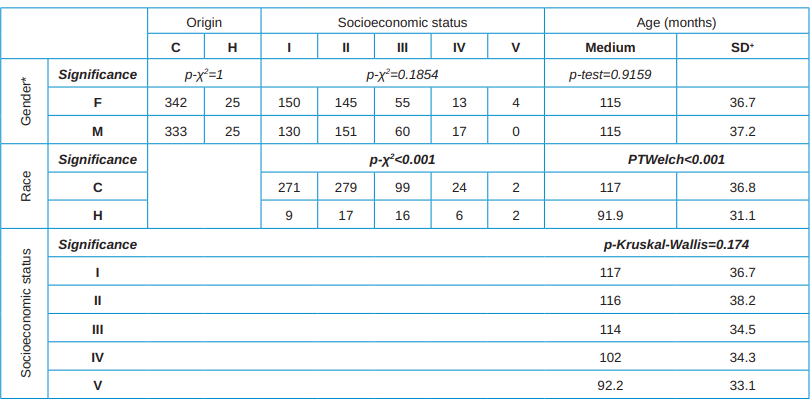
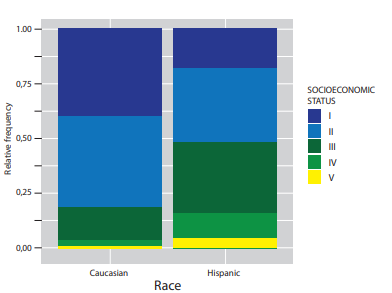
Data were recorded from 725 individuals (367 girls and 358 boys). 93.1% of the sample was of Caucasian origin and the remaining 6.9% was of Hispanic origin. Regarding the socioeconomic status, 38.62% belonged to a level I, 40.83% to level II, 15.86% to a level III, 4.14% to a level IV and 0.55% to a level V. Statistically significant differences were found between socioeconomic status and patient origin: Caucasian subjects had better socioeconomic status. No significance was observed in the distribution of socioeconomic status regarding gender and age. (Table 1, Figure).
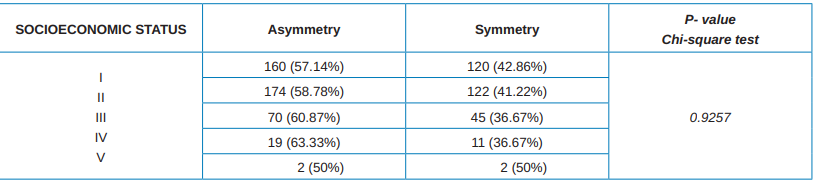
The eruption symmetry was presented in 41.38%, being significantly higher the percentage of subjects without symmetry (68.62%) (p-χ2 <0.001). The presence of symmetry in the upper arch was significantly related to that of the lower arch (p-χ2<0.001), being present in 67.87% of the children. Asymmetry in the upper and lower arch simultaneously was found in 71.38% of the sample. No significant results were found in the relationship between sex and eruption symmetry (p-χ2=0.582) or between race and symmetry (pχ2=0.5901). There was also no significance between eruption symmetry and socioeconomic status (pχ2=0.9257) (Table 2).
A univariate logistic regression model was carried out, finding that sex, race and socioeconomic status were not predictors of eruption symmetry (p-Wald>0.05 in all analyses). On the other hand, age was found to behave as a significant predictor variable, p-Wald=0, OR (odds ratio)=1.02718806.
The first permanent tooth to appear in the maxilla was the first molar (74.34-76.41%) and in the mandible the central incisor (78.9-82.76%), with statistically significant differences (p-χ2<0.001). The symmetry and emergence of the first tooth was analysed, there was only a significant relationship between symmetry and the fourth quadrant (p-fisher=0.003391), since when erupting there was asymmetry in 80.95% of the cases.
When analysing the relationship between the eruption of the first tooth and the study variables, the socioeconomic status did not show statistically significant differences in any quadrant (p-Fisher>0.05 in all cases). With respect to sex and race, the data were significant for gender and lower-right hemiarch and race and upper left hemiarch. In girls the first tooth to erupt in the fourth quadrant was the central incisor (98.01%) (p-Fisher=0.04563), and in Caucasian boys the emergence in the second quadrant was the first permanent molar (98.65%) (p-Fisher=0.01365).
The eruption symmetry and sex were predictive variables regarding the emergence of the first tooth in the lower-right hemiarch (p-Wald=0.007 and p-Wald=0.046, respectively), and the race in the first and second quadrant (maxillary arch) (p-Wald<0.05). Age was a predictive p-wald<0.05 in all quadrants.
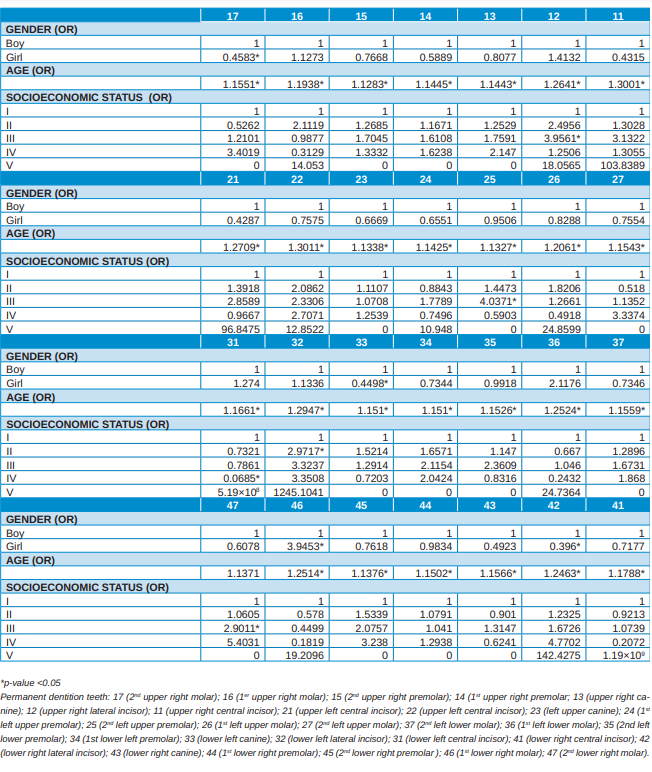
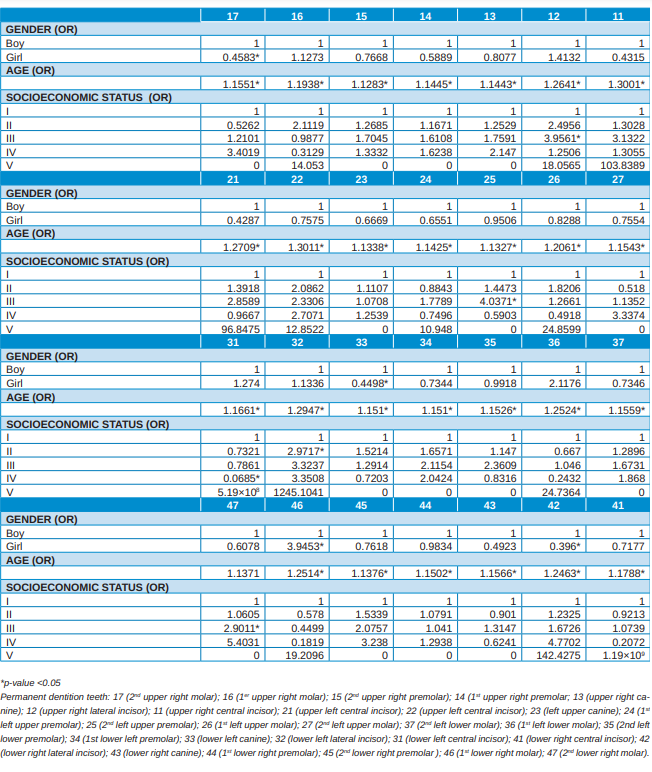
Sex was found to be significant in the eruption of the 17, 33, 42 and 43 teeth since the probability of eruption was higher in boys regarding tooth 46 whose probability was higher in girls (Table 3).
Knowing the chronology and eruption sequence of permanent dentition is essential as an improvement in treatment planning at both preventive paediatric dentistry or orthodontic level16. In this regard, Veloso et al. associated the eruption sequence and motor laterality function17.
Current changes in the emergence chronology are relevant for forensic dentistry. Several authors insist on the differences in chronological and sequential level of the eruption according to race or geographical area12,18. Schmeling et al. highlighted the influence of the various ethnic groups in the procedures that existed for estimating the age of the patient and the difficulty that appeared in cases in which the population of the studied subject had no reference19 studies.
According to Nassif and Sfeir, premolars and second molars emerge at an early stage in Lebanese children compared to established standards20. Therefore, knowing the eruptive population characteristics is relevant at forensic level regarding identification cases in war conflicts, migratory movements, refugee flows or accidents of any type3,21.
Regarding sex, several authors indicate that in girls the emergence is at an earlier stage, due to hormonal causes20-26. Saenz Martinez et al. observed this characteristic, except for tooth 464. In our research, teeth 17, 33, 42 and 43 are more likely to emerge in boys compared to girls, while teeth 46 emerge earlier in girls. According to Vithanaarachchi et al., the exception lies in the central incisors27. However, Oz and Kirzioglu note that the eruption in girls is earliest at age 5, but in groups of 6-8 years and 10-12 years there would be no statistically significant differences regarding sex28.
Almeida et al., in their research, also corroborated the earliest eruption in girls than boys, the upper teeth erupting between 4.3 and 4.4 months before and the lower teeth between 3.0 and 3.729. Valenzuela et al.
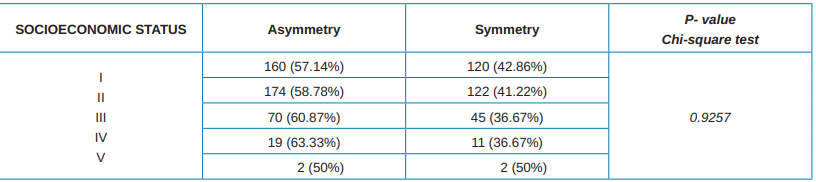
symmetry/ asymmetry of permanent dentition and its
relationship with socioeconomic status. Contingency table and
chi-square test.
exception of wisdom teeth.
also observed an earlier eruption in girls compared to that of boys, as did Gonzalez et al.30,31 Plasencia et al., in their study in Spain, and Dahiya et al., in India, highlighted the same eruption pattern, being this earlier in females than in males32,33.
Regarding the socioeconomic status, there is no consensus, since early emergence is associated with children with higher socioeconomic levels or the opposite34.35. In our study, we found no significance between symmetry, eruption chronology and socioeconomic status. According to Clements et al., at a higher socioeconomic status better medical care, better nutrition and earlier emergence of permanent teeth, except for the second premolar, since the latter is more susceptible to caries and, therefore, to present an earlier exfoliation and a later eruption of its successor34.
On the contrary, Dimaisip-Nabuab et al. believe that a lower socioeconomic status and worse nutrition favour the presence of untreated caries pathology and delayed eruption36. Phillips et al. suggested that a high socioeconomic status could play an important role in the calcification of permanent teeth influencing x-rays vision used to detect the age of the individual37.
In relation to the sequence the first tooth to emerge when the purchasing level is higher, are the mandible incisors, while in population with less resources the first mandible molars35 erupt first. In our research, no statistically significant differences were found in this regard, observing how in the first quadrant the probability of the lateral incisor emerging was approximately four times greater for individuals of social class III. The same would occur in the second quadrant with the second premolar. At the third quadrant level, the probability of the lateral incisor appearing was multiplied by three for social class II and by fifteen for the central incisor appearing for social class IV. Finally, at the fourth quadrant level the piece 46 would have a probability of emerging three times higher for the social class III. Colomé et al. emphasize in their study that the first tooth to emerge is also the lower central incisor, followed by the first lower molar38. However, Valenzuela et al. determined that the first tooth to erupt in its structure was the first molar both upper and lower30.
Regarding the racial factor, in our study the chronology of eruption of the permanent dentition was faster in those individuals of Hispanic origin than in those of
Caucasian origin and the probability of symmetry was multiplied by 2.5 for individuals of Hispanic origin. In addition, there was a significant relationship in the second quadrant with the origin of the child, that is, the first tooth to erupt predominated more in individuals of Hispanic origin than in those of Caucasian origin.
Debrot, in his research, also concludes that the teeth emerged earlier in black race than in white39 race, just like Mugonzibwa40, Kutesa41 and Hassanali42 that pointed out that the eruption in African and African American children was faster than that of Asians and Caucasians. Coinciding with our results, Steggerda et al. concluded that there were differences in the eruption times according to the races, erupting before in the Navajo race, then in the black race, then in the Mayan race and finally in the white race43. Colomé et al. observed that the eruption chronology of the population of southeastern Mexico was late with respect to that reported in Anglo-Saxon studies and early with respect to the population of central Mexico38.
In reference to the limitations of our research, it should be noted that a larger sample with individuals with a lower socioeconomic status would enrich the obtained results. Since it is not a longitudinal study, it is not possible to determine if there are changes regarding the eruption and sequence in the same patient. However, we highlight as strengths the diversity of results regarding sex and the chronology and sequence, noting that, today, establishing a strict norm in terms of these variables is complex, since the eruption chronology and sequence depend on multiple factors. Therefore, future studies will be necessary to endorse the obtained results.
In conclusion, regarding gender, significance was observed for some teeth in males and in girls only a significance in the emergence of the lower right first molar. Regarding the socioeconomic status, this does not influence the chronology or the eruption sequence of permanent dentition.


Muñoz Cano, Laura
Graduated in Dentistry from the Complutense University of Madrid (UCM). Master in Pediatric dentistry and Interceptive Orthodontics from the European University of Madrid (UEM). PhD student UEM.
Paz Cortés, Marta Macarena
Paediatric dentistry. Specialist in children with special needs UCM. Doctor in Dentistry UCM. Paediatric dentistry Professor in the Dentistry Degree of Alfonso X El Sabio University (UAX). Master Paediatric dentistry Professor UCM.
Dieguez Perez, Montserrat
Paediatric dentistry. Specialist in children with special needs UCM. Doctor in Dentistry UCM. Paediatric dentistry Professor in the Dentistry Degree UEM. Master Paediatric dentistry Professor UCM
Indexed in:
- IME (Spanish Medical Index)
- IBECS (database)
- LATINDEX (Regional Online Information System)
- GOOGLE ACADEMIC