Puesta al día
Regeneración ósea con injertos intraorales: rama vs. mentón. Puesta al día
La utilización de injertos intraorales en bloque es una alternativa de tratamiento válida para la regeneración en anchura de defectos óseos maxilares y mandibulares. Sin embargo, actualmente no hay consenso entre los diferentes autores en la elección del mejor tipo de bloque intraoral a utilizar. Por ende, esta puesta al día busca comparar la ganancia ósea, la tasa de complicaciones postoperatorias y el éxito del injerto entre bloques autólogos de rama mandibular y mentón.
La ganancia ósea alcanzada es similar en ambos bloques. No obstante, se podría deducir una mayor ganancia al utilizar bloques de la rama mandibular cuando son evaluados mediante CBCT. Además, la tasa de reabsorción ósea fue menor con los injertos de rama.
La supervivencia de los implantes es equiparable con ambos tipos de injertos.
Las complicaciones que tienen lugar, en orden de frecuencia, son las alteraciones sensoriales, las necrosis pulpares, dehiscencias y hemorragias; apareciendo con mayor frecuencia en los bloques de mentón. Además, el periodo de recuperación en las zonas de rama mandibular es más lento.
De este modo, a la hora de la elección parece razonable individualizar el caso y tener en consideración aspectos como la morbilidad y el acceso a la zona donante.
The use of intraoral block grafts is a valid treatment alternative for the regeneration of maxillary and mandibular horizontal bone defects. However, there is currently no consensus among different authors on the choice of the best type of intraoral bone block to use.
Therefore, this update seeks to compare bone gain, post-operative complication rate and grafting success between autologous mandibular ramus and chin bone block grafts.
The bone gain achieved is similar in both block grafts. However, a higher gain can be observed by CBCT when using mandibular ramus blocks. In addition, the rate of bone resorption is lower with ramus grafts.
Implant survival is comparable in both types of grafts.
The complications that occur, in order of frequency, are sensory alterations, pulp necrosis, dehiscence and bleeding, appearing more frequently in chin blocks. In addition, the recovery period in the mandibular ramus areas is slower.
Thus, when choosing, it seems reasonable to individualize the case and take into consideration aspects such as morbidity and access to the donor area.
Las extracciones dentarias producen una reabsorción horizontal y vertical de la cresta ósea, que se acentúa por motivos periodontales, endodónticos y/o traumáticos. Esta reabsorción ósea produce un limitado volumen de hueso alveolar residual, que conduce a un compromiso estético y funcional, y que dificulta el éxito del tratamiento implantológico posterior. Como consecuencia, existen procedimientos regenerativos; como los injertos óseos en bloque, la regeneración ósea guiada y la distracción alveolar1 .
La regeneración ósea en bloque es una técnica de aumento óseo horizontal y/o vertical con resultados predecibles y estabilidad a largo plazo2 . Los bloques óseos empleados en regeneración ósea horizontal pueden ser autólogos, heterólogos y alogénicos3 . El hueso autólogo se considera, hoy en día, el gold standard debido a sus propiedades de osteogénesis, osteoconducción y osteoinducción. No obstante, presenta una mayor morbilidad para el paciente y una disponibilidad limitada4 . Su origen puede ser intra o extraoral, en función de la necesidad de volumen óseo, la tasa de reabsorción y la morbilidad de la zona donante. Las zonas donantes extraorales más frecuentemente empleadas son la cresta iliaca o la diáfisis tibial. En cuanto a las zonas intraorales destacan la zona retromolar, seguida de la región sinfisaria y en ocasiones, la tuberosidad maxilar2,5.
Además, estos injertos difieren considerablemente en cuanto a la embriología (membranosos o endocondrales), la histología y las propiedades mecánicas4 .
La obtención de injertos intraorales presenta ventajas frente a los extraorales, como la accesibilidad quirúrgica, la proximidad de la zona donante y receptora y una menor morbilidad6 . Sin embargo, hoy en día no hay consenso entre los diferentes autores entre el tipo de bloque intraoral a utilizar en regeneración ósea horizontal.
Por tanto, el objetivo de la presente revisión es comparar la ganancia ósea, la tasa de complicaciones postoperatorias y el éxito del injerto, tras la reconstrucción de la cresta alveolar con injertos autólogos en bloques procedentes de la rama mandibular frente a los del mentón.
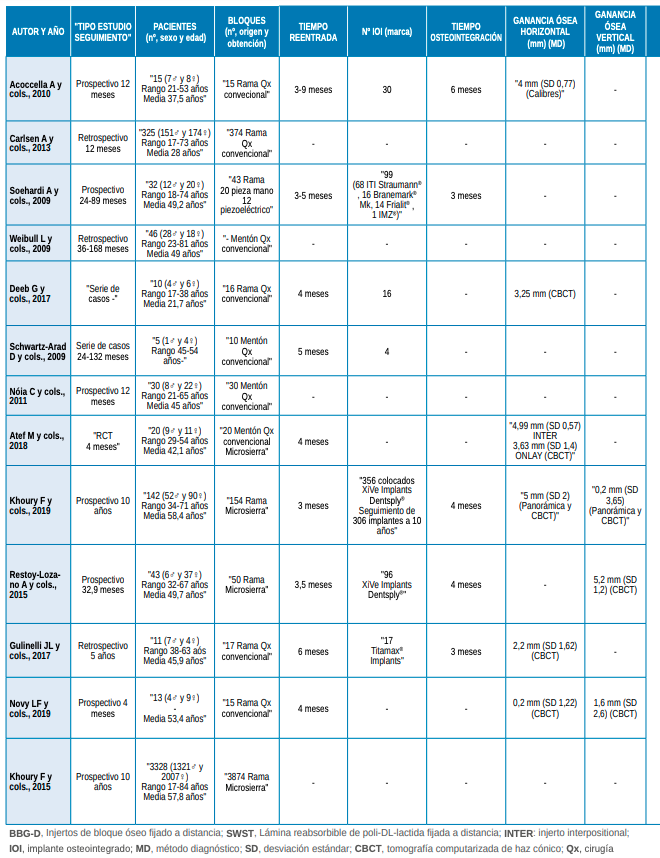
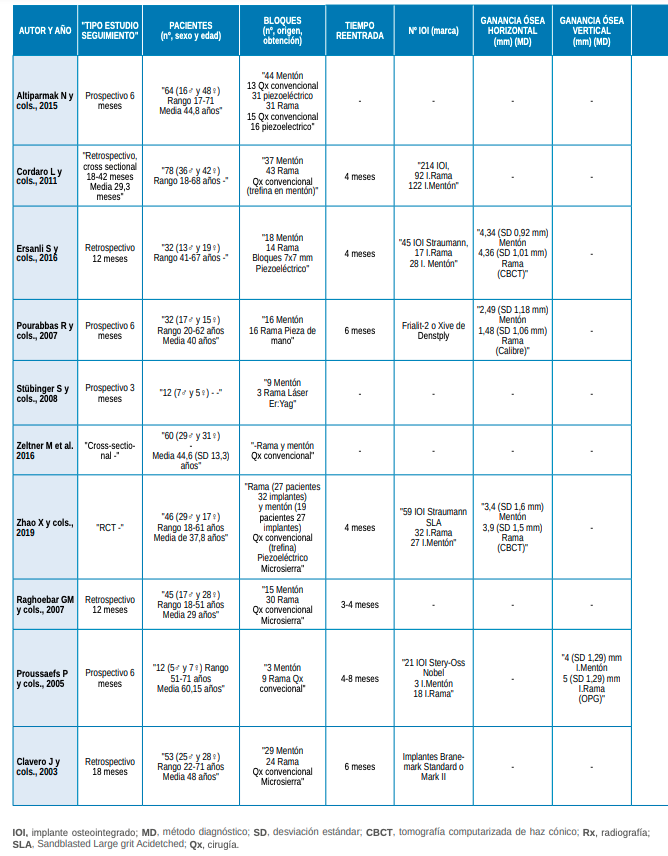
Se incluyeron un total de 23 estudios clínicos, los cuales registraron 5051 bloques injertados y 957 implantes colocados en 4454 pacientes. 13 estudios fueron de una sola cohorte, en los que se analizaron 106 bloques de mentón y 4558 de rama, procedentes de 4020 pacientes a los que se les colocaron 618 implantes (Tabla 1). Los 10 estudios restantes compararon 190 bloques procedentes de mentón y 197 de rama en 434 pacientes, a los que se les colocaron 339 implantes (Tabla 2).




Los estudios incluidos evaluaron la ganancia ósea en anchura con diferentes métodos de medición: calibres, radiografía panorámica y tomografía computarizada de haz cónico (CBCT).
Los datos procedentes de los estudios de una sola cohorte obtuvieron entre 0,2-5 mm de ganancia ósea horizontal al emplear injertos de rama7-11, respecto a los 4,31 mm medidos a través de CBCT, alcanzados con los bloques de mentón12.
Los estudios comparativos obtuvieron una ganancia evaluada con CBCT comprendida entre 3,4-4,34 mm para los injertos de mentón, mientras que para los de rama, ésta fue de 3,9-4,36 mm13,14. En cambio, al utilizar calibres, la ganancia resultante para los injertos de mentón fue de 2,49 1,18 mm frente a 1,48 1,06 mm para los injertos de rama15.
No obstante, es más fiable la determinación de la anchura ósea mediante CBCT. En resumen, se apreció una mayor ganancia con los bloques procedentes de la rama mandibular al ser medidos mediante CBCT13,14. Sin embargo, empleando el método de calibres se observa una mayor ganancia utilizando los injertos de mentón15.
Con respecto a la ganancia en altura, los estudios de una sola cohorte evaluados mediante CBCT y radiografía panorámica, obtuvieron valores comprendidos entre 0,2-5,2 mm al emplear injertos de rama8,10,16. En cambio, el estudio comparativo de Proussaefs y cols.,17, indica un valor medio de 4 mm al emplear injertos de mentón y de 5 mm con los de rama.
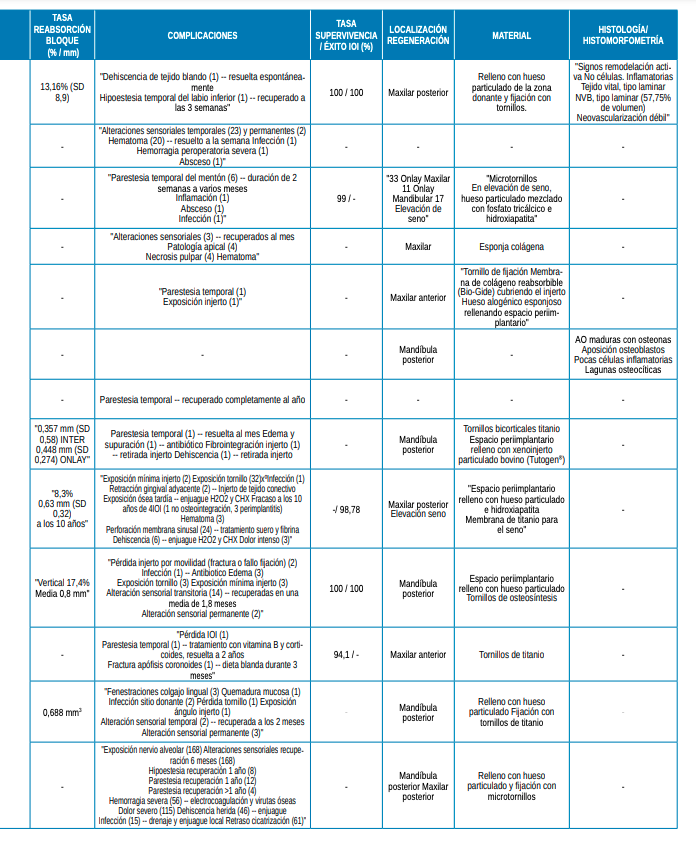
Los estudios revisados evaluaron la reabsorción de los bloques mediante el CBCT. 5 de los 13 estudios de una cohorte evaluaron la tasa de reabsorción, estando comprendida entre 8,3-17,4% para los bloques de rama7,8,10,16 y alrededor de 5,27% para los bloques de mentón12.
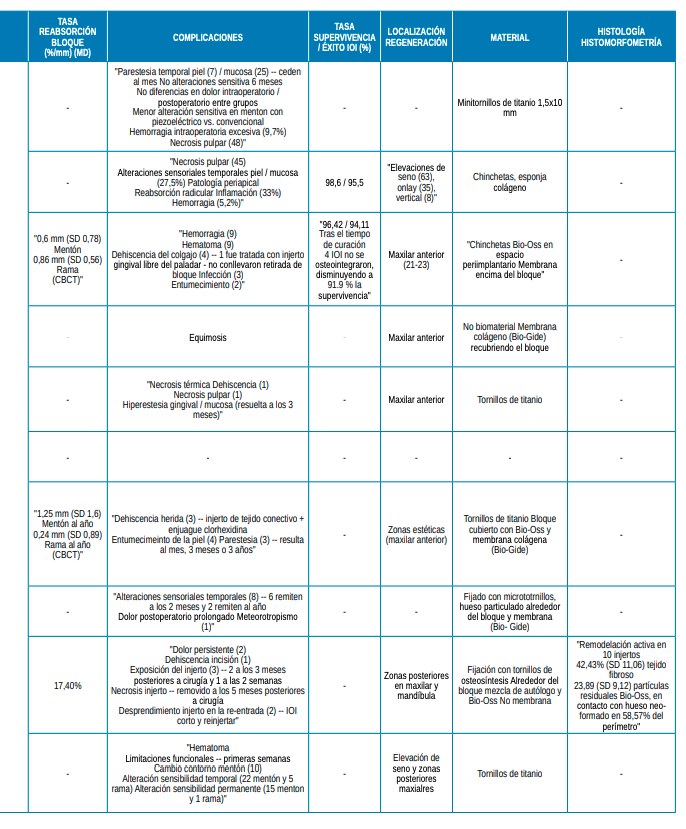
En los estudios comparativos, sólo 3 de ellos aportan datos sobre la reabsorción producida en los bloques. Los 37 injertos de mentón alcanzaron una reabsorción comprendida entre 0,6-1,25 mm al año de colocar los bloques; mientras que, en los 41 bloques de rama, fue de 0,24-0,86 mm al año. Además, el estudio de Proussaefs y cols.,17 indica una tasa global de reabsorción del 17,4% a lo largo de 6 meses, para 9 bloques de mentón y 3 de rama.
Se podría confirmar que los injertos de rama sufren una menor reabsorción con respecto a los de mentón13,14. Esto podría verse justificado debido a que los injertos de rama están constituidos fundamentalmente por hueso cortical, el cual presenta una menor cantidad de células osteogénicas y, por tanto, una menor reabsorción. En cambio, los injertos esponjosos se reabsorben más rápidamente debido a la estructura y microarquitectura que presentan18.
Los estudios de una sola cohorte mostraron tasas de supervivencia comprendidas entre 94,1-100%, en 242 implantes con un seguimiento entre 12 meses y 5 años7,11,16,19.
Solo dos estudios comparativos mostraron tasas de supervivencia, que oscilaron entre 91,9-98,6% tras un tiempo de seguimiento entre 12-42 meses. Cordaro y cols.,20, observaron una tasa de supervivencia total de 98,6% en 214 implantes, de los cuales 92 fueron colocados en una zona rehabilitada con injerto de rama y 122 en una zona con injerto de mentón. En el estudio de Ersanli y cols.,13, tras la colocación de 45 implantes, 17 de ellos en la zona injertada con bloque de rama y 28 en la zona tratada con injerto de mentón, la tasa supervivencia fue de 96,42% en un periodo de 4 meses, y de 91,9% en un periodo de 12 meses. De este modo, ambas zonas injertadas presentaron tasas de supervivencia implantológica similares.
Comparando los estudios de forma global, el empleo de membrana colágena cubriendo los bloques fue utilizado en 6 de los 23 estudios clínicos8,9,13-15,21. El uso de ésta confirma una disminución de la tasa de reabsorción del bloque, así como menores complicaciones, tal y como se observó en los estudios de Khoury y cols.8 y Restoy-Lozano y cols16.
Además, en 10 de los 23 estudios incluidos, como los de Atef y cols.12, Ersanli y cols.13 y Zhao y cols.14, entre otros, el espacio periimplantario se rellenó con hueso particulado autólogo y heterólogo (Bio-Oss), favoreciendo la cicatrización. Esto aporta ventajas particulares en zonas de demanda estética, dado que este material facilita el apoyo para el tejido blando. Además, su porosidad y superficie conducen a una mejor respuesta osteogénica, al dar soporte a la formación de nuevos vasos sanguíneos y al depósito de nuevo hueso; y la tasa de reabsorción es más lenta18.
En los 13 estudios de una sola cohorte, se obtuvieron 16 complicaciones diferentes de 4020 intervenciones, lo correspondería a una probabilidad de 0,39% de sufrir alguna complicación tras cada intervención quirúrgica7-12,16,19,22-26.
De las diversas complicaciones, las más frecuentes han sido las alteraciones sensoriales temporales, seguidas de la dehiscencia de la herida y el hematoma. Sin embargo, estas complicaciones no supusieron la retirada del bloque injertado y consecuentemente el fracaso del tratamiento. Las 221 alteraciones sensoriales que tuvieron lugar, 216 en 4404 bloques de rama (4,90%) y 5 en 53 bloques de mentón (9,43%), se resolvieron espontáneamente, con vitamina B o corticoides; no obstante, 7 de 221 (3,17%) no revirtieron en los bloques de rama y se consideraron permanentes tras el paso del primer año.
Por otro lado, para las 60 dehiscencias ocurridas en 4129 bloques, se utilizaron enjuagues de clorhexidina y peróxido de hidrógeno8,11. Como consecuencia de esta complicación, cabe mencionar la retirada de un bloque de mentón, tal y como refiere el estudio de Atef y cols.,12.
Con respecto a los 10 estudios comparativos, se obtuvieron un total de 11 complicaciones diferentes6,13-17,20,21,27-29. En un total de 387 bloques, tuvieron lugar 98 alteraciones sensoriales temporales (25,32%), 94 necrosis pulpares (24,29%) y 20 hemorragias excesivas intraoperatorias (5,17%)6,13,20. Cabe mencionar que, de las 98 alteraciones neurosensoriales ocurridas, 16 de ellas (15 en mentón y 1 en rama) (16,33%) se volvieron permanentes tras año y medio27.
De los 23 estudios incluidos, 2 de ellos no registraron complicaciones. La complicación más frecuente fue la alteración sensitiva temporal, cuya recuperación varió entre las 2 semanas y los 24 meses; y como complicaciones menos frecuentes, caben mencionar el meteorotropismo (sensibilidad al tiempo atmosférico), descrito en el estudio de Raghoebar y cols.,21, y la fibrointegración del injerto con su consecuente retirada, en el estudio de Atef y cols.,12.

Pérez López, Carmen
Odontóloga por la Universidad Complutense de Madrid (UCM), Máster Oficial en Ciencias Odontológicas (UCM).
Bazal Bonelli, Santiago
Alumno del Magíster en Cirugía Bucal e Implantología UCM.
Sánchez-Labrador, Luis
Magíster en Cirugía Bucal e Implantología UCM.
Díaz Olivares, Luis Alfredo
Máster Oficial en Ciencias Odontológicas UCM.
Valdés Álvarez, Armando
Máster Oficial en Ciencias Odontológicas UCM.
Madrigal Martínez-Pereda, Cristina
Codirectora Magíster Cirugía Bucal e Implantología UCM.
López-Quiles, Juan
Director Magíster Cirugía Bucal e Implantología UCM.
Indexada en / Indexed in: – IME – IBECS – LATINDEX – GOOGLE ACADÉMICO