Puesta al día
Material de injerto en elevación de seno de acceso lateral: ¿es necesario? Parte II
Introducción: Las extracciones dentarias producen una reabsorción del proceso alveolar en sentido horizontal y vertical además de la neumatización del seno. Estos cambios óseos en la zona posterior del maxilar pueden comprometer la colocación de implantes. La técnica convencional o de acceso lateral sigue siendo la técnica más utilizada para realizar elevaciones de seno maxilar. Estas elevaciones se realizan tanto sin injertos óseos como con diferentes biomateriales. Existe cierto debate sobre si es necesario colocar o no injerto.
Objetivo: Analizar y comparar la ganancia ósea en elevaciones de seno de acceso lateral con injerto y sin injerto.
Material y método: Se realizó una búsqueda electrónica para la actualización del tema en tres bases de datos y una serie de libros relacionados.
Resultados: Se obtiene una ganancia de 4,0-6,14 mm cuando no se emplea material de injerto y entre 3,11-13,1 mm cuando se emplean biomateriales. Los estudios reflejan una pérdida ósea marginal entre 1,01-1,9 mm cuando no se emplea material de injerto y 2,3 mm de media cuando se emplean biomateriales. La técnica de elevación de seno de acceso lateral sin empleo de biomaterial presenta unas tasas de supervivencia elevadas pero las tasas de supervivencia son ligeramente superiores cuando se emplean biomateriales. La tasa de complicaciones es baja para ambas técnicas, siendo la más frecuente la perforación de la membrana de Schneider, que no parece suponer un impedimento para la colocación de implantes.
Conclusión: la técnica de elevación convencional con relleno obtiene mayor ganancia ósea, pero mayor pérdida ósea marginal y presenta una tasa de supervivencia alta de implantes en comparación con la técnica que no emplea material de injerto, por lo que se debe individualizar cada caso para decidir si es necesario o no la utilización de un sustituto óseo.
Introduction: dental extractions produce a resorption of the alveolar process, horizontally and vertically in addition to pneumatization of the sinus. These bone changes in the posterior area of the maxilla can compromise implant placement. The conventional or lateral access technique is still the most used technique to perform maxillary sinus elevations. These elevations are performed without bone grafts and with different graft biomaterials where there is some discussion whether or not it is necessary to place a graft.
Objective: Analyze and compare bone gain in graft and non-graft lateral access sinus lifts.
Material and method: An electronic search was carried out to update the subject in three databases and a series of related books.
Results: A gain of 4.0-6.14 mm is obtained when no graft material is used and between 3.11-13.1 mm when biomaterials are used. Studies show a marginal bone loss between 1.01-1.9 mm when no graft material is used and 2.3 mm on average when biomaterials are used. Lateral access sinus elevation technique without the use of biomaterial has high survival rates but survival rates are slightly higher when biomaterials are used. Rate of complications is low for both techniques, the most frequent being the perforation of Schneider’s membrane, which doesn’t seem to be an impediment to the placement of implants.
Conclusion: conventional lift technique with filling obtains greater bone gain, but greater marginal bone loss and presents a high implant survival rate compared to the technique that doesn’t use graft material, so each case must be individualized to decide if it’s necessary or not the use of a bone substitute.
Las extracciones dentarias producen una reabsorción del proceso alveolar, en sentido horizontal y vertical, que en la zona posterior del maxilar puede comprometer la colocación de implantes, haciendo necesaria la realización de cirugías regenerativas adicionales, como es la elevación de seno maxilar1-3.
La elevación de seno maxilar mediante técnica convencional o ventana lateral, descrita por Boyne y James4 , es la técnica de elección en casos con altura ósea residual menor a 4 mm y sigue siendo la técnica más empleada para llevar a cabo elevaciones de seno maxilar5 . Según el protocolo original, se realiza un colgajo a espesor total mediante una incisión supracrestal que permita visualizar la pared lateral del seno maxilar que, con una posterior osteotomía, se retira o se eleva hacia la cavidad sinusal6-8. El procedimiento de elevación del seno maxilar se ha realizado con diferentes materiales de injerto (injertos óseos autógenos, aloinjertos y xenoinjertos) y sin material de injerto, produciéndose formación de hueso nuevo alrededor del implante9-11 .
El objetivo del presente artículo es comparar la utilización de diferentes materiales de injerto en elevaciones de seno de acceso lateral o convencionales con la no utilización de éstos, evaluando la ganancia ósea, la pérdida ósea marginal, la tasa de supervivencia implantaria y la aparición de complicaciones.
2.1. Objetivo principal Analizar y comparar la ganancia ósea en elevaciones de acceso lateral con injerto y sin injerto.
2.2. Objetivos secundarios
- Analizar y comparar la pérdida ósea marginal en elevaciones de seno de acceso lateral con injerto y sin injerto.
- Analizar la tasa de supervivencia para ambas técnicas.
- Analizar la tasa de complicaciones para ambas técnicas.
- Comparar las elevaciones de acceso lateral de seno sin injerto con las que sí se emplea injerto, determinando las ventajas e inconvenientes.
3.1. Criterios de inclusión
- Estudios clínicos aleatorizados en humanos, estudios prospectivos, estudios retrospectivos, a propósito de un caso y series de casos.
- Estudios clínicos en los que se incluyan comparación de procedimientos de elevación de seno con colocación de implantes con injerto y sin injerto.
- Estudios clínicos en los que se incluyan procedimientos de elevación de seno con colocación de implantes sin injerto.
- Estudios publicados en inglés.
- Estudios de los últimos 20 años.
3.2 Criterios de exclusión
- Estudios en animales.
- Estudios in vitro.
- Estudios de elementos finitos.
- Ensayos clínicos en los en los que el artículo no estuviese disponible.
3.3. Fuentes y estrategia de búsqueda
Se realizó una búsqueda electrónica en tres bases de datos: The National Library of Medicine (MEDLINE/ Pubmed); Web of Science, y SCOPUS. La búsqueda incluyó estudios publicados en inglés y español con restricción de fecha de publicación de los últimos 20 años. Además, se realizó una búsqueda manual en revistas y libros de Cirugía Oral y Maxilofacial. Para las bases de datos Pubmed, Web of Science y Scopus, la estrategia de búsqueda fue en modo avanzado sin filtros:
1# (graftless [All Fields] AND (paranasal sinuses [MeSH Terms] OR (paranasal [All Fields] AND sinuses [All Fields]) OR paranasal sinuses [All Fields] OR sinus [All Fields] OR sinus s [All Fields]) AND (lifting [MeSH Terms] OR lifting [All Fields] OR lift [All Fields]).
2# (graft s[All Fields] OR grafted [All Fields] OR graftings [All Fields] OR transplantation [MeSH Subheading] OR transplantation [All Fields] OR grafting [All Fields] OR transplantation [MeSH Terms] OR grafts [All Fields] OR transplants [MeSH Terms] OR transplants [All Fields] OR graft [All Fields]) AND (paranasal sinuses [MeSH Terms] OR ( paranasal [All Fields] AND sinuses [All Fields]) OR paranasal sinuses [All Fields] OR sinus [All Fields] OR sinus s [All Fields]) AND (lifting [MeSH Terms] OR lifting [All Fields] OR lift [All Fields]).
3.4 Artículos seleccionados
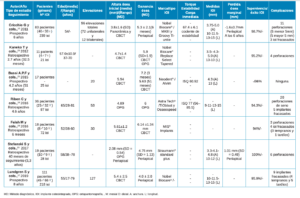
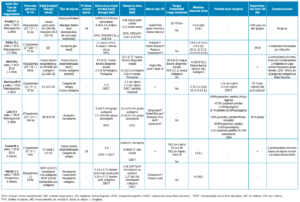
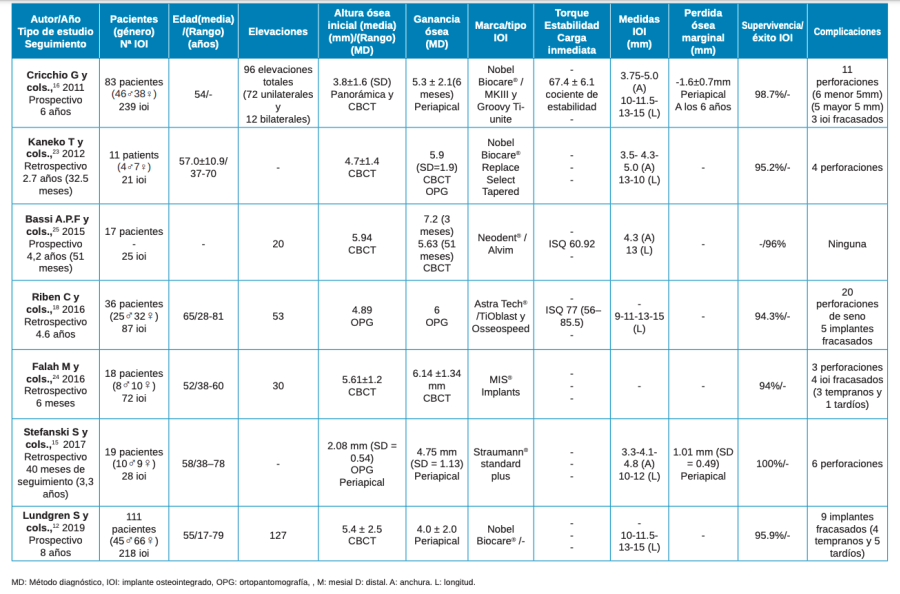
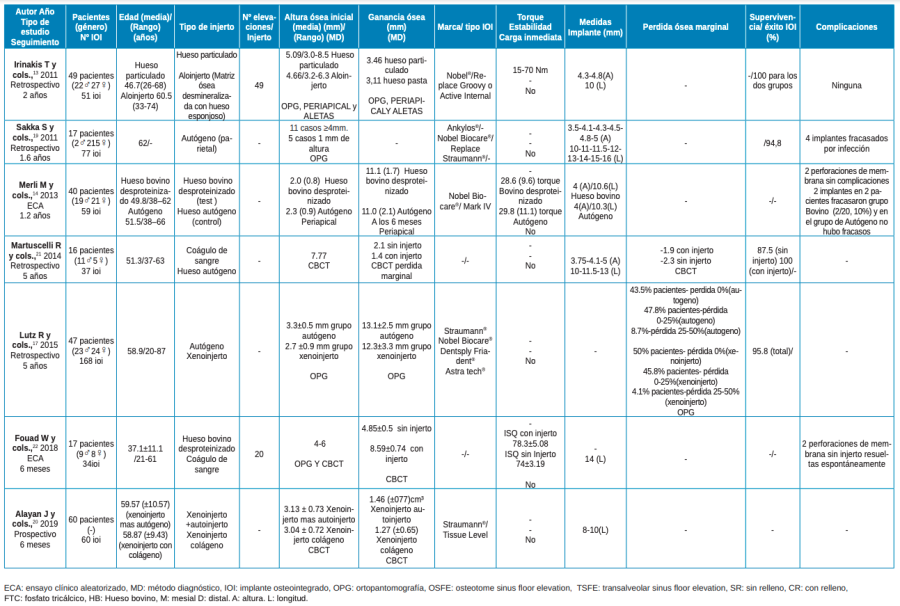
Se incluyeron un total de 14 estudios clínicos de los últimos 9 años en los que se colocaron un total de 1176 implantes en 541 pacientes. En 7 de los 14 estudios se describieron elevaciones de seno de acceso lateral sin colocación de material de injerto, evaluando 690 implantes en 295 pacientes (Tabla 1). En los otros 7 estudios se comparó la técnica de elevación de acceso lateral empleando y sin emplear material de injerto, colocándose 486 implantes en 246 pacientes (Tabla 2).
4.1. Ganancia ósea
Los estudios revisados evaluaron la ganancia ósea mediante radiografía periapical, panorámica y tomografía computarizada de haz cónico (CBCT) disponiéndose de la siguiente manera:
4.1.1. Radiografía periapical
Los estudios en los que se utilizó la radiografía periapical como método para evaluar la ganancia ósea tras la elevación de seno de acceso lateral fueron 5. En 3 de estos 5 estudios no se colocó material de injerto y en los otros 2 se compararon distintos tipos de injertos entre sí (aloinjerto de tipo particulado, aloinjerto en presentación con jeringa, hueso autógeno y xenoinjerto de origen bovino)12,13. En cuanto a los estudios que realizaron elevaciones de seno sin emplear material de injerto, se analizaron 485 implantes, obteniéndose una ganancia ósea de entre 4,0-5,6 mm14-16.
En 2 de los estudios sin injerto se utilizaron paralelizadores a la hora de llevar a cabo las radiografías14,15, mientras que en 1 no se registró16. En los estudios donde se compararon injertos entre sí, en 1 de ellos si se utilizó paralelizador13 mientras que en el otro no se usó12. En los 2 estudios comparativos entre diferentes materiales, se colocaron 110 implantes y se comparó la colocación de aloinjerto y xenoinjerto de origen bovino, registrando una ganancia de 3,11-11,0 mm cuando se empleó material de injerto de origen humano y entre 3,46-11,1 mm al emplear injerto de origen animal12,13.
4.1.2. Radiografía panorámica
Los estudios en los que se evaluó la ganancia ósea mediante radiografía panorámica tras la elevación de seno de acceso lateral fueron 3. En 1 de ellos no se empleó material de injerto y en 2 de ellos se compararon diferentes materiales de injerto. Los materiales comparados fueron xenoinjerto particulado de origen bovino, aloinjerto (matriz ósea desmineralizada de hueso esponjoso) y hueso autógeno12,17. En el estudio en el que no se empleó material de injerto, se analizaron 87 implantes, con una ganancia ósea vertical media de 6 mm18. En los 2 estudios comparativos, se colocaron 219 implantes, obteniendo una ganancia ósea de entre 3,11-13,1 mm en el grupo de hueso autógeno y 3,46- 12,3 mm en grupo de xenoinjerto bovino12,17,19 .
4.1.3. Tomografía computarizada de haz cónico (CBCT)
6 estudios evaluaron la ganancia ósea tras la elevación de seno de acceso lateral mediante CBCT. En 3 de ellos no se utilizó material de injerto y en otros 3 estudios se comparó la utilización o no de material de injerto, entre los que encontramos xenoinjerto de origen bovino y hueso autógeno20-22. En los 3 de estudios de elevaciones sin injerto se analizaron 118 implantes, obteniendo una ganancia ósea vertical de 5,6-6,14 mm23-25. Los otros 3 estudios comparativos evaluaron 131 implantes, obteniendo una ganancia ósea de 2,1- 4,85 mm en el grupo sin material de injerto, respecto a 1,4-8,59 mm al emplear xenoinjerto de origen bovino y hueso autógeno20-22 .
4.1.4. Ganancia ósea global
Al comparar los artículos de forma global, se obtuvo una ganancia ósea de 4,0-6,14 mm sin emplear materiales de injerto14-16,18,23-25; 3,46-12,3 mm cuando se empleó material de injerto de origen animal12,17,20-22; y 3,11-13,1 mm cuando se empleó material de injerto de origen humano.
4.2. Pérdida ósea marginal
Los estudios revisados evaluaron la pérdida ósea a lo largo del tiempo mediante radiografía periapical, radiografía panorámica y CBCT.
4.2.1. Radiografía periapical
Los estudios en los que se utilizó la radiografía periapical como método para evaluar la pérdida ósea marginal tras la elevación de seno de acceso lateral fueron 2, siendo elevaciones de acceso lateral sin injerto en ambos casos. En estos dos estudios se colocaron 267 implantes, con una pérdida ósea marginal de entre 1,01-1,6 mm con un seguimiento de 3,3-6 años14,15. Estas radiografías se realizaron mediante el uso de paralelizadores.
4.2.2. Radiografía panorámica
Un estudio evaluó con radiografía panorámica la pérdida ósea marginal, comparando distintos tipos de injerto. Se midió la pérdida en porcentajes, obteniéndose una pérdida del 0% en el 43,5% de los pacientes totales donde se usó hueso autógeno y en el 50% de los pacientes totales donde se usó xenoinjerto. En el 47,8% de los pacientes con hueso autógeno y en el 45,8% de los pacientes con xenoinjerto se obtuvo una pérdida de entre 0% y 25%. En el 8,7% de los pacientes con hueso autógeno y en el 4,1% de los pacientes con xenoinjerto se obtuvo una perdida de entre 25% y 50%17.
4.2.3. Tomografía computarizada de haz cónico (CBCT)
Sólo 1 estudio comparativo evaluó la pérdida ósea marginal en elevación de acceso lateral mediante CBCT. Se observó una pérdida ósea media de 1,9 mm cuando se utilizó hueso autógeno y 2,3 mm cuando no se utilizó material de injerto21.
4.2.4. Pérdida ósea global
Comparando los artículos de forma global, se obtuvo una pérdida ósea marginal media de 1,01-1,9 mm en implantes colocados mediante elevaciones de seno con acceso lateral sin emplear material de injerto14,15,21 y de 2,3 mm cuando se usó como biomaterial hueso autógeno21.
4.3. Supervivencia de los implantes
Los estudios de elevación de seno sin relleno mostraron tasas de supervivencia de entre 94-100%, con un seguimiento de 6 meses-8 años14-16,18,23-25. Los estudios comparativos presentaron tasas de supervivencia del 87,5-95,8% cuando no se emplearon materiales de injerto y del 95,8-100% cuando sí se emplearon biomateriales asociados, con un tiempo de seguimiento de 6 meses-5 años12,13,17,19,20-22
4.4. Complicaciones
En los 7 estudios en los que se analizaron elevaciones de seno de acceso lateral sin emplear material de relleno se obtuvieron un total de 44 complicaciones siendo, en todos los casos, la perforación de la membrana de Schneider. Estas perforaciones no supusieron un impedimento para completar la cirugía14,15,18,23,24. Aunque la complicación más frecuente fue la perforación de la membrana de Schneider, en ningún paciente se produjo patología infecciosa en el seno maxilar. Con respecto a los 7 estudios comparativos, solo hubo 4 complicaciones , siendo todas ellas perforaciones de la membrana de Schneider y resueltas de manera espontánea13,22. De los 14 estudios revisados, 2 de ellos no registraron ninguna complicación12,25.
En el abordaje lateral de elevación de seno, los implantes dentales se pueden colocar de manera simultánea, con o sin injertos óseos19. El hueso autólogo es el material de elección dadas sus propiedades osteoinductoras, osteoconductoras y osteogénicas pero su uso está limitado por la morbilidad en el sitio donante26. Independientemente del biomaterial empleado en esta técnica, sus resultados son predecibles según la literatura científica. Esto podría ser explicado por el hecho de que el seno maxilar tiene un gran potencial para la formación de hueso y que un material de injerto no es un requisito previo para esta formación27.
En uno de los estudios analizados, donde no se emplea material de injerto, se constató que se puede formar hueso nuevo directamente alrededor de los implantes. Se consiguen ventajas como un ahorro notable de tiempo en la cirugía y en el coste económico en vez de utilizar biomateriales23,24. Para conseguir una formación ósea predecible sin injerto, varios autores enfatizan en que la cantidad de espacio del seno rellenado con coágulo de sangre supone un paso importante. El efecto de tienda de campaña de los implantes que se produce en la membrana, probablemente depende de la longitud de los implantes16,23.
Comparando la altura del hueso basal inicial se logró una estabilidad primaria aceptable en prácticamente todos los casos, a pesar de contar con una altura inicial disponible de menos de 4 mm. La posición apical del injerto en la elevación parece favorecer dicha estabilidad14,19. Por otro lado, se relaciona el diseño del implante con una mayor estabilidad primaria, dando a entender que el propio relleno en sí no daría estabilidad alguna13. En elevaciones de acceso lateral sin injerto, en cambio, en todos los estudios analizados la altura ósea media inicial va desde los 2 hasta los 8 mm y fue posible también insertar todos los implantes con una estabilidad primaria adecuada. Lo que se puede sugerir es que la altura ósea residual mínima para retener un implante es de 4 mm13,14,19.
Hay que tener en cuenta que se produce una mayor reabsorción en los materiales de injerto, como reflejan los resultados obtenidos en 2 estudios, donde se observan pérdidas volumétricas de material del 45,7% con el hueso autógeno28 o del 36,71% con el xenoinjerto29.
En todos los estudios la perforación de la membrana es la complicación más frecuente, aunque no supuso un impedimento para la colocación de los implantes y tampoco hubo una diferencia aparente en la ganancia ósea obtenida, comparando los que no tuvieron ninguna complicación frente a los que si tuvieron13-15,18,22-24. Por lo tanto, la elevación del seno maxilar es un procedimiento seguro, que combina altas tasas de supervivencia del implante y baja incidencia de complicaciones quirúrgicas17.
- La ganancia ósea obtenida mediante la elevación de seno de acceso lateral varía entre 4,0-6,14 mm cuando no se emplea material de injerto y entre 3,11-13,1 mm cuando se emplean biomateriales.
- La perdida ósea marginal obtenida varía entre 1,01-1,9 mm cuando no se emplea material de injerto y es de 2,3 mm de media cuando se emplean biomateriales.
- La técnica de elevación de seno de acceso lateral sin empleo de biomaterial presenta unas tasas de supervivencia elevadas. Cuando se emplean biomateriales, las tasas de supervivencia son ligeramente superiores.
- La tasa de complicaciones es baja para ambas técnicas, siendo la más frecuente la perforación de la membrana de Schneider, que no parece producir patología infecciosa en el seno maxilar.
- El empleo de biomateriales obtiene mayor ganancia ósea, pero mayor pérdida ósea marginal y presenta una tasa de supervivencia alta de implantes en comparación con la técnica que no emplea material de injerto. Parece razonable, según los estudios consultados, individualizar cada caso para decidir si es necesario o no la utilización de un sustituto óseo para la colocación simultánea de implantes en técnicas de elevación de seno de acceso lateral.

Valdés Álvarez, Armando
Odontólogo por la Universidad Alfonso X El Sabio (UAX), alumno del Máster en Cirugía Bucal e Implantología Universidad Complutense de Madrid (UCM).
Pérez López, Carmen
Alumna del Máster en Cirugía Bucal e Implantología UCM.
Bazal Bonelli, Santiago
Alumno del Máster en Cirugía Bucal e Implantología UCM.
Sánchez-Labrador, Luis
Profesor del Máster en Cirugía Bucal e Implantología UCM.
Cobo Vázquez, Carlos
Profesor del Máster en Cirugía Bucal e Implantología UCM.
Meniz García, Cristina
Profesora contratada doctora de Cirugía Bucal. Profesora del Máster en Cirugía Bucal e Implantología UCM.
Indexada en / Indexed in: – IME – IBECS – LATINDEX – GOOGLE ACADÉMICO