Clinical case
Block grafting in combination with the two-stage split technique for the rehabilitation of a case of severe bone resorption of the maxilla in width
The use of different surgical techniques to achieve the resolution of the most complex atrophy cases is of vital importance.
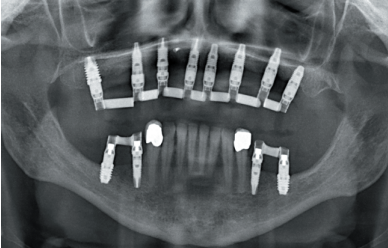
Increasingly, we have cases with edentulism of longer duration in our practice that require implant treatment with fixed prosthesis, which is a challenge when planning and carrying out treatments. To do this, we can use different techniques that allow us to gain width and height, as well as implants of different lengths and diameters that allow us to adapt to each situation. In the present clinical case, we show a rehabilitation that combines different surgical techniques to achieve the desired result.
More and more frequently, patients with long-term edentulism, wearing complete prosthesis come for dental consultation requesting implantology treatment. The digital age, social networks and patient access to clinical information in dentistry, means that the latest advances in rehabilitation of extremely atrophic maxillary and mandible reach the patients and they demand a solution to their situation, they thought it could not be corrected in any other way than with removable dentures1-4. Therefore, patients sometimes request implantology treatments in cases of great complexity that make us have to use all the surgical and prosthetic tools at our disposal to solve them5.
When we face a severe resorption in a horizontal sense, both in the maxilla and in the mandible, there are different techniques that help us to recover the lost bone volume to later insert dental implants6-7. Each of the techniques has its indications and may, sometimes, in the same patient, need several of these techniques to achieve a regeneration of the lost bone volume, since there are substantial variations in the quality and quantity of bone volume within the same arch of the same patient, as well as areas where in addition to width the bone plates have been completely or partially lost, which changes the approach of the technique to employ6-9.
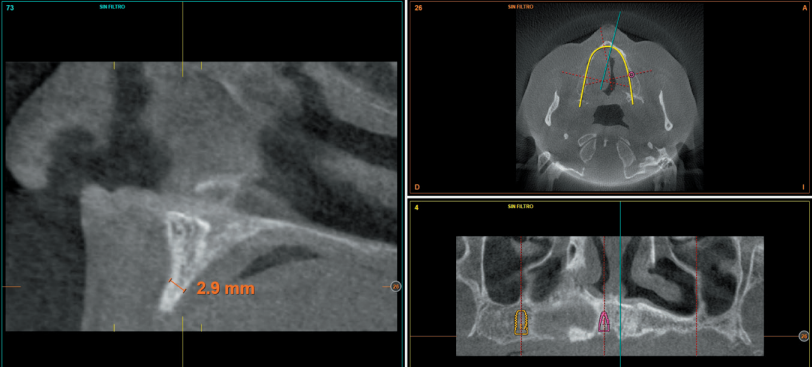
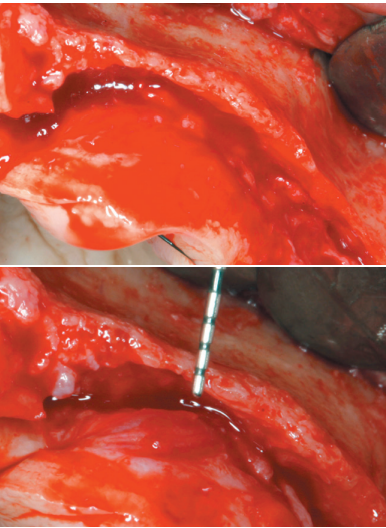
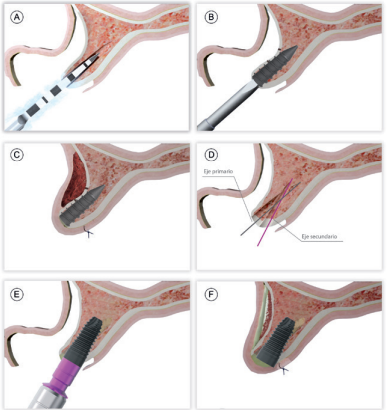
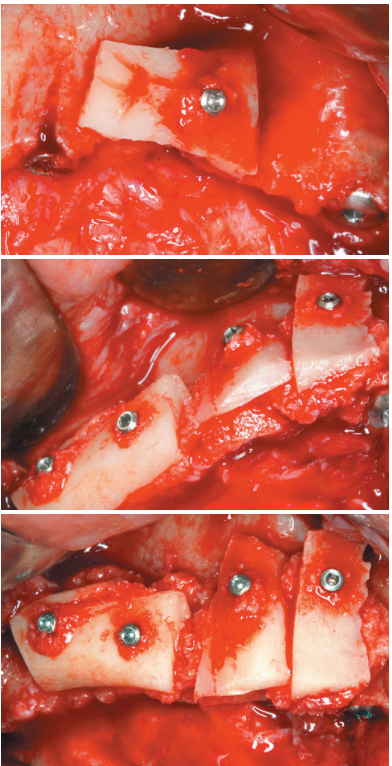
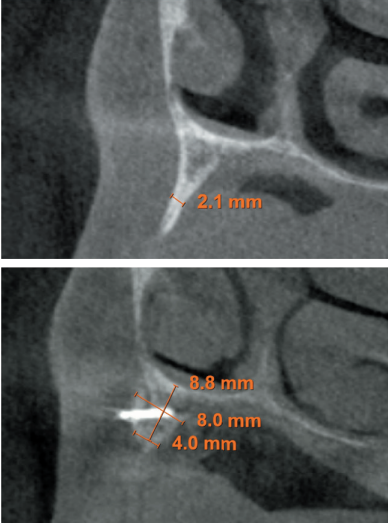
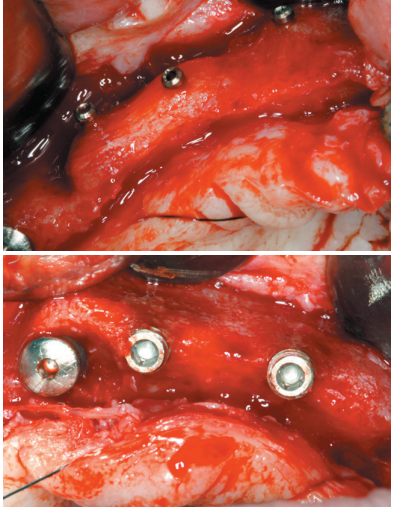
In general, when there is a reduced bone width (below 3 mm of residual crest) that does not allow direct insertion of the implant we can opt for an expansion or split crest, in one or two phases, as long as the two bone plates are available and there is a bone particulate between them that allows the separation between them by inserting the definitive implant or the expander implant10-14. When one of the two bone plates is absent, in that case, the recommendation will be to use block grafts or guided bone regenerations13-14.
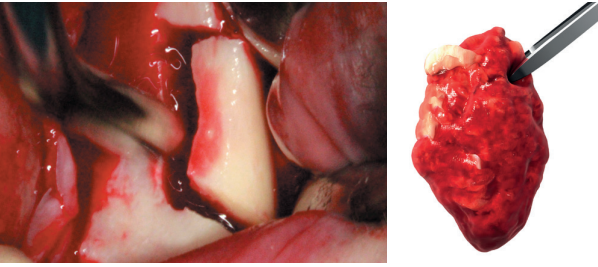
Both techniques are widely documented15, and the selection between one procedure and the other is mainly based on the availability of autologous bone to perform block surgery, and the ability of the operator to perform the technique, since the use of blocks requires a greater learning curve and can lead to more complications in obtaining, manipulating and healing, since it is a technique of greater technical difficulty.
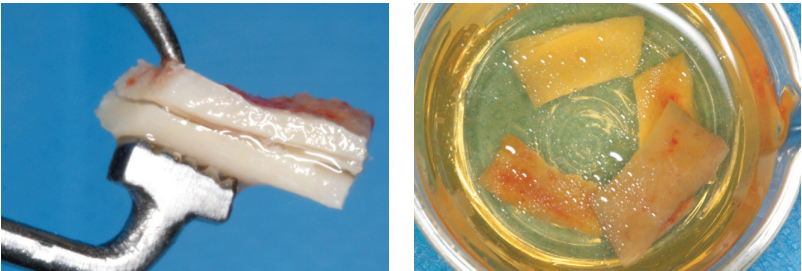
In spite of all this, if careful protocols are used to obtain the graft, and a careful positioning technique is performed, paying special attention to soft tissues, nowadays, it can be performed without greater rate of complications than the bone regeneration technique, especially when the intraoral area is used as the donor zone and the obtained bone is maximized by dividing the block as described by Khoury16-18.
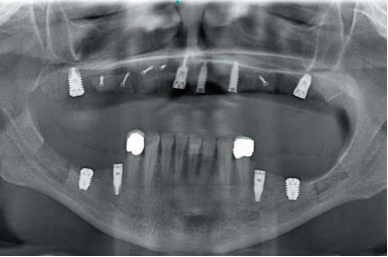
In the following clinical case, a situation is shown where different procedures have been necessary to rehabilitate the maxilla with extreme bone loss in width, depending on each of the areas to be treated, individualizing the type of treatment according to the characteristics of the remaining bone recess.