Original article
Radiographic diagnosis of impacted maxillary canines: Comparison between two and three dimensions
Introduction: An impacted canine is a very common condition and raises several clinical complications. Early and exact diagnosis is important in order to minimise the risks and subsequent complications. The objective of this study is to analyse the effectiveness of two dimensions in the volumetric diagnosis for impacted maxillary canines, using the lines proposed by Alqerban as a reference.
Methods: An orthodontic study of the maxilla using orthopantomography with cone beam computed tomography (CBCT) at the Madrid European University Clinic was performed on 27 patients selected with 36 maxillary impacted canines. Three reference lines were drawn based on the distance from the cusp of the canine to the occlusal plane (L1), to the midline (L2) and to its ideal eruption site (L3), in both the orthopanthomography and the CBCT. As ideal reference values, we selected a control group of 36 erupted maxillary canines.
Results: The results were compared in 2 and 3 dimensions using the Student’s t test, after verifying their normal distribution using the Anderson-Darling contrast test. Statistical significance (p > 0.05) was not obtained for any of the variables studied.
Conclusions: The use of CBCT is vital to ensure good diagnosis of the canine position and its relationship with adjacent structures and thus establish an adequate treatment plan. However, orthopantomography provides sufficient information for initial planning.
Canines are of vital importance in facial and oral aesthetics, as well as in the functionality and development of occlusion. Both Andrews1 with his six keys to occlusion and the latest articles by Clark2 demonstrate the importance of the canine in occlusion. There is no doubt that the canine is one of the pillars in the ideal occlusion scheme proposed by nature. If it is in an aberrant position, it can cause alterations in the entire occlusion system. Due to its anatomy, the maxillary canine guides mandibular movements and supports the forces of occlusion, with a large crown compared to the size of the mandibular tooth itself, and is the tooth with the greatest stability. Its roots are the longest and widest, so these teeth have a firm anchorage in the alveolar bone. Clinically, canines are the teeth that should be lost last. Due to their strategic location in the mouth, they are the cornerstones of the dental arch3 .
The maxillary canine is the permanent tooth with the longest eruption path. It begins forming with a mesial tilt and rapid growth, then slows down as it straightens or even shows a slightly distal diversion.4 This change in speed and inclination corresponds to the contact of the canine with the distal area of the lateral incisor, at approximately 9 years of age. Hence the important role played by the upper lateral incisor in the eruption of the canine. The prevalence and incidence of an impacted maxillary canine is widely reported in the literature. The earliest articles we found in this regard were by Cramer in 19295 and Mead in 19306 . These describe an incidence of 1.4% and 1.57%, respectively, after selecting a sample of American white males. Other authors expand and modify the sample, and obtain prevalences of 0.92% (Dachi7 ), 1.8% (Thilander and Jakobsson8 ), 2.2% (Thilander and Myberg9 ), 3.61% (Aitasa- lo10) and 2.8% (Ericson and Kurol4,11-13).
For the interarch position, the classification refers to maxillary canines impacted by the palatal or vestibular. According to this classification14, Jacoby found that 92.31% of patients (a ratio of 12:1) had a palatal impaction, on later expansion of the sample, a ratio of 6.6:1, palatal vs vestibular, was found. Other authors, such as Gaulis and Joho15 obtained a ratio lower than 2:1. The international consensus is for a ratio of 3:1. The current classification, proposed by authors such as Stivaros and Mandall16, reduces the percentage of palatal inclusions to 61%, while vestibular inclusions appear in 5% of patients. For these authors, 34% of canines would be positioned at an intermediate point in the arch. For Rimes et al,17 the proportion of canines impacted palatally is 44%, while those displaced in the vestibular position is 38%. Syrynska18, however, reported 60.3% for palatal canines and 20.6% for vestibular; while 19.2% were in an intermediate position in the alveolus.
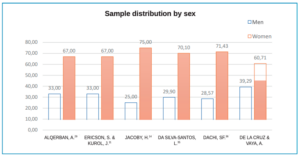
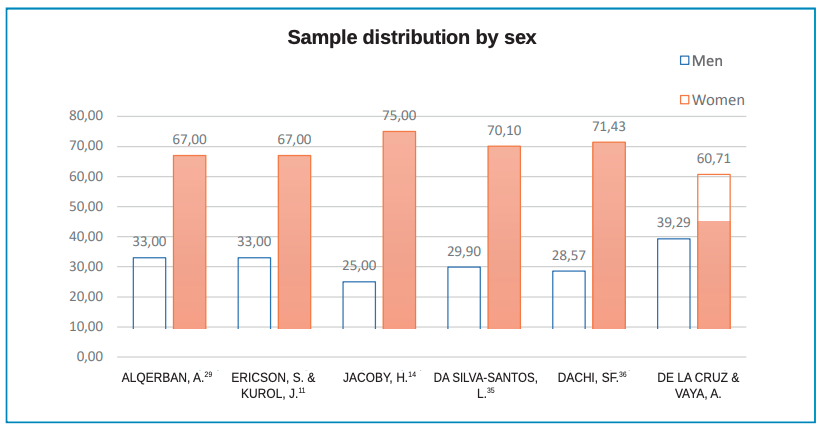
The literature suggests impaction occurs more in women than men. Dachi7 reports 78.57%, Gashi19 77.10% and Bishara20 suggests a ratio of 2:1 for maxillary canine impaction in women over men, which is confirmed by Cooke21.
Regarding bilaterality, 8% of patients have a bilateral impaction according to Dachi7 , Bishara20, Manne22 and Yadav23. Shirazi24, however, found no association in gender for unilateral or bilateral impaction in maxillary canines.
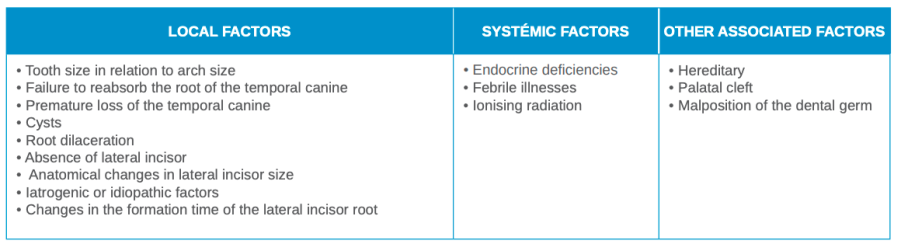
Most authors associate palatal inclusion with the Caucasian race, at 5.9%, while vestibular inclusion is associated with Asians, 1.7%25-27. The impaction ratio of Caucasian patients to African or Asian patients is 2:1, according to Peck and Peck28. Etiological factors associated with impacted canines are shown in Table 1.

A total of 148 patients (76 men and 72 women) with one or both maxillary canines impacted were selected from those who underwent orthodontic studies during the Master’s of Orthodontics at the University Clinic between 2009 and 2016.
The inclusion criteria were as follows: patients with impacted upper uni- or bilateral canines; over 10 years old of either sex; with a diagnostic CBCT and orthopantomography of the maxilla. The following were excluded: those with previous completed orthodontic treatment; those with agenesis or absence of one or both upper canines; agenesis or absence of one or both upper central incisors; agenesis or absence of one or both upper first premolars; syndromic patients or those with medical complications, including metabolic and/or endocrine disturbances related to eruption alterations.
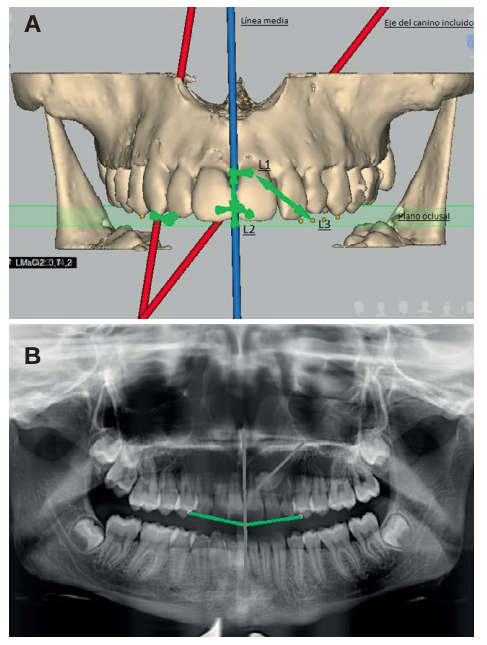
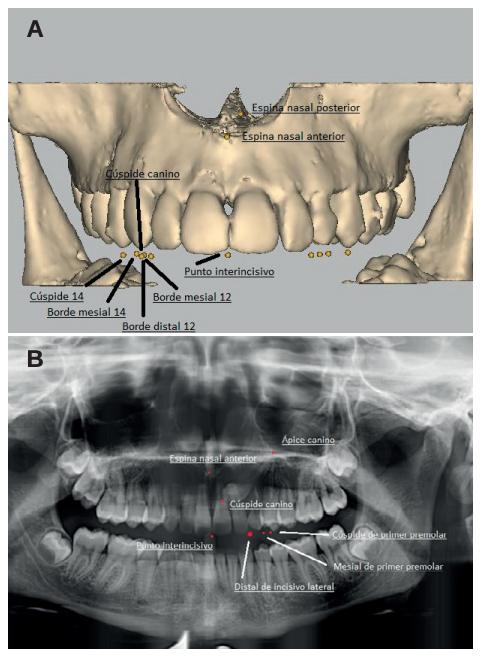
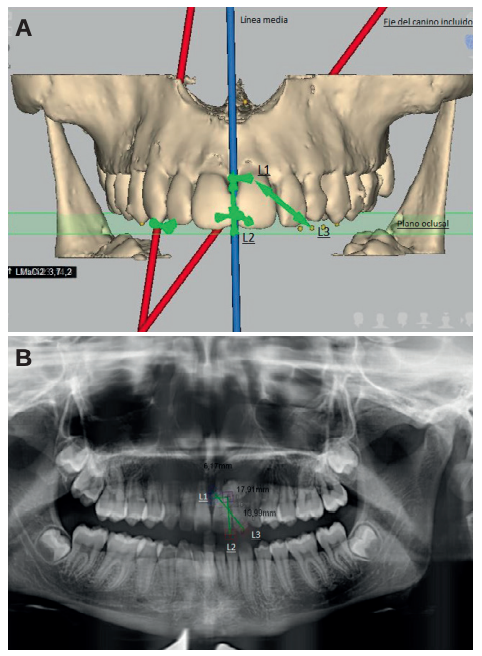
A sample of 28 patients with 36 impacted maxillary canines was selected after applying the inclusion and exclusion criteria. The CBCT and orthopantomography scans performed during the orthodontic study were then analysed and a new cephalometric tracing was created by a single investigator using Nemotec 3D software. In this analysis, a series of dental and skeletal points of reference were created and selected, both in the orthopantomography and in the CBCT, upon which planes and measurement axes were drawn according to the Alqerban method29 . Three linear distances were measured from the cusp of the canine using these points, planes and axes: to the occlusal plane (L1); to the midline (L2); and to the canine’s ideal eruption site (L3), as described in Figures 1-3 for both diagnostic methods.
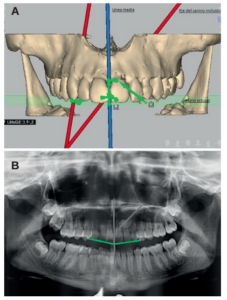
Figure 1B. Measurements, axes and planes in orthopantomography.

Figure 2B. Points marked in orthopantomography.
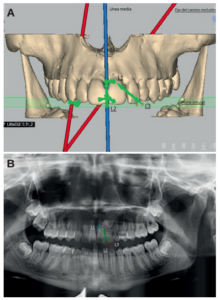
Figure 3B. Reference lines in orthopantomography.
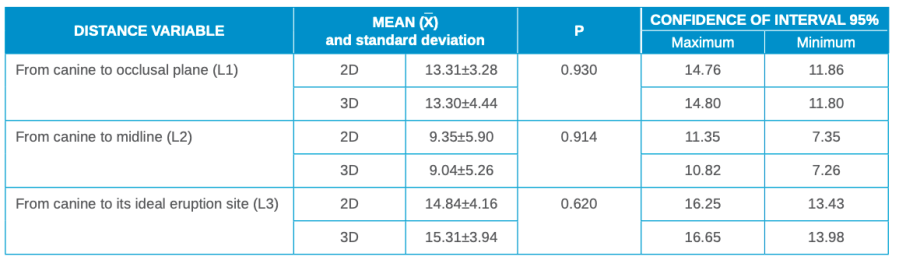
A descriptive data analysis of the variables L1, L2 and L3 was carried out in 2 and 3 dimensions using the mean, standard deviation and confidence intervals.
From these data and applying the Anderson-Darling contrast test of normality, the normal distribution of the sample was observed. The results of the radiographic methods in 2 and 3 dimensions were compared by means of the Student’s t test for the difference of means.
The stati sti cal analysis results for the mean, p value and confidence interval are summarised in millimetres in Table 2. As can be seen in Table 3, no statistically significant differences were obtained at a value of p < 0.05 for any of the three variables studied (L1, L2 and L3).
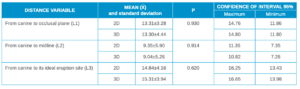
Of the three variables, L1 showed less deviation between 2D and 3D, with similar values for both. On the other hand, L2 tended to overesti mate the values obtained in 2D, if it is considered that 3D measurements are “real or gold standard”. The 2D values for the variable L3 tended to underesti mate those in 3D. The difference in the variables prevented any att empt at obtaining a mathematical formula to calculate the degree of deviation for these measurements for any of the variables.
An impacted tooth is a pathological condition defined by its failure to erupt in the oral cavity within the ti me and conditions considered normal for it, based on clinical and radiographic diagnostic methods. The radiographic method of choice for initial diagnosis is orthopantomography.
However, panoramic radiography does not always provide us with all the necessary information for a proper diagnosis and planning of the case. According to Ericson and Kurol30, panoramic radiography is not sufficient for the detection of impacted teeth, with additional diagnostic radiographic methods being necessary.
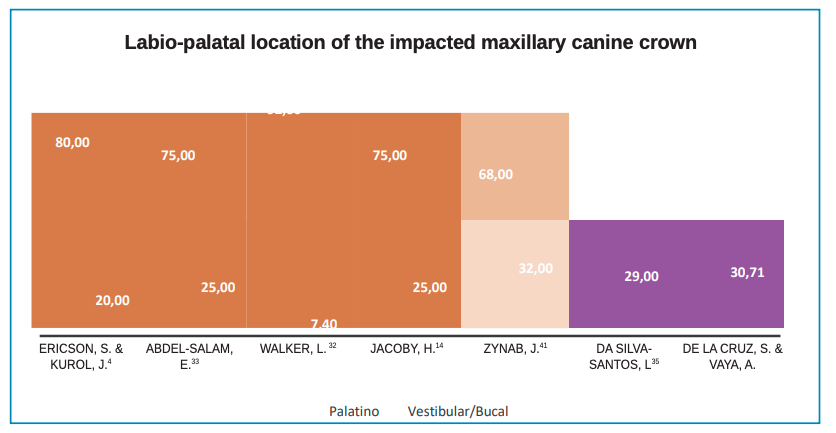
Regarding prevalence, in the study of 28 pati ents, 11 (39.29%) were men and 17 (60.71%) women. This gives us a greater number of pati ents included in the female sample with a rati o slightly lower than the 2:1 proposed by Ericson and Kurol30 or the 78.9% proposed by Walker in 200531, as shown in Figure 4. All the authors consulted obtained results similar to those seen in the classic articles, with a ratio of approximately 2:1. This ratio has been associated for years with population density, the eruptive sequence and early bone growth in females. Regarding the canine deviation trajectory, 65% of these were located palatally, which is lower than that proposed by other authors such as Walker30, or Ericson and Kurol32, with palatal impaction percentages of 80% and 91%, respectively; as shown in Figure 5.
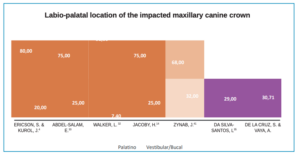
As confirmed in Figure 4, all authors agree that palatal displacement of the canine is more frequent in Caucasian pati ents. All the samples taken in the preparation of Figure 4 refer to Caucasian, AfricanAmerican or African pati ents. For the Asian population, there is apparently a greater predisposition to impaction vestibularly over palatally, for an as yet unknown reason34.
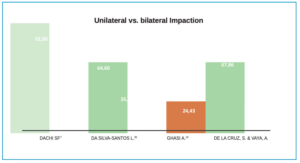
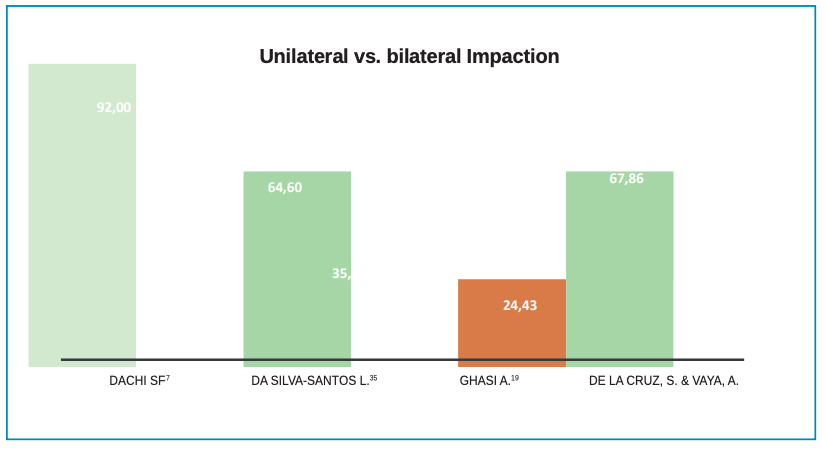
Finally, the present study gave values of 67.86% for unilateral impactions, which is similar to those obtained by Da Silva-Santos35, and clearly lower than those obtained by Dachi in 196136 and as compiled by Bishara in 199220, as shown in Figure 6.
The values for impacted canines are similar to those obtained by Alqerban. For the distance from the cusp of the canine to the midline, Alqerban obtained a mean value of 9.60 mm, while, the mean in our sample was 7.62 mm; for the distance of the impacted canine to the occlusal plane, Alqerban had a mean distance of 10.60 mm compared to 12.67 mm in our sample. Due to its condition and eruptive trajectory, the maxillary canine is a major risk factor in root resorption of the lateral incisor, so its early diagnosis not only lies in avoiding impaction of the canine, but also plays an important role in avoiding lateral incisor injury. As Stivaros demonstrated in his 2000 study37, 2.3% of canines deviate their eruption in a higher position than normal, which is a risk factor and an indicator of lateral incisor root reabsorption.
This study shows that, compared to the 2-dimensional method, the CBCT provides us with information and clear images of the intraosseous position, inclination, morphology of the impacted tooth and the proximity and relationship of the impacted maxillary canine with various anatomical structures and root dilacerations that cannot be detected with the 2D radiographic method, as stated by Chen2 , Sawamura38 and Walker39 in their studies.
As we have mentioned in the results section and following, the difference in the lines and measurements proposed by Alqerban, and transferred to an orthopanthograph as a reference, are not statistically significant (p > 0.05), which indicates that the linear measurement performed in a CBCT or in an orthopantomography would provide the same result. For more accuracy, the data from a larger sample size would have to be studied, since our sample size is not comparable to that of other authors mentioned.
Although the diagnostic advances in image processing in recent years with CBCT represent a great advance in dentistry and, in this case, in orthodontics, the ideal diagnostic method for each pati ent must be chosen individually. The choice of radiographic method to be used depends on the type of treatment to be performed. With new advances, the 3-dimensional technique can select specific regions of the face, thus minimising the amount of radiation. These advances represent a double-edged sword when it comes to updating protocols and systems, since clinicians need to update their 3-dimensional knowledge to offer patients optimal treatment and diagnosis40.
In evaluati ng the linear positi on of the impacted maxillary canine, orthopantomography provides suffi cient informati on for initi al planning of the case, without giving clear informati on on the relati onship of the canine to the adjacent structures. However, CBCT remains the method of choice for diagnosing the linear and angular positi on of the impacted maxillary canine. This study represents a fi rst phase in the diagnosis and planning of the treatment, with angular measurements needing to be introduced to determine the degree of impacti on of the maxillary canine, as well as to predict the diffi culty of treatment.

Vayá Fernández-Ladreda, Alberto
Graduate in Dentistry from Alfonso X El Sabio University. Master’s Degree in Advanced Orthodontics from the European University of Madrid.
De la Cruz Vigo, Susana
Doctor of Dentistry and a professor for the Master’s in Advanced Orthodontics at the European University of Madrid.
Indexed in: – IME – IBECS – LATINDEX – GOOGLE SCHOLAR