Revisión bibliográfica
Escobar Bores P, Peña Salguero PM, Arias Macías C. Influencia de la masticación unilateral no alternante en el desarrollo maxilofacial y tratamiento precoz. Cient. Dent. 2023; 20; 2; 119-128
Influencia de la masticación unilateral no alternante en el desarrollo maxilofacial y tratamiento precoz
Resumen
Introducción: La masticación unilateral no alternante es un hábito nocivo consistente en realizar la masticación de forma exclusiva o predominante por uno de los dos lados de la dentición que, mantenido en el tiempo durante el crecimiento, origina un desarrollo asimétrico del complejo craneofacial afectando a las estructuras óseas, musculares, articulares y dentarias.
Objetivo: Describir cómo influye la masticación unilateral en el crecimiento maxilofacial y en la oclusión, así como el abordaje precoz para evitar las consecuencias de este hábito.
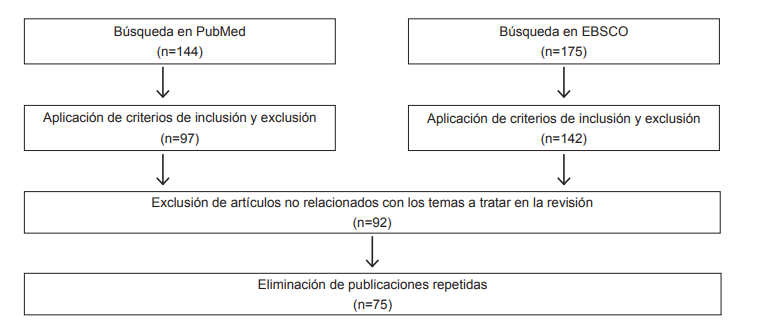
Material y método: Se realizó una búsqueda bibliográfica en el metabuscador EBSCO-Dentistry Oral Science Source y en PubMed, seleccionando artículos a texto completo en inglés y español relacionados con el tema, de lo que se extrajeron 45 para realizar esta revisión.
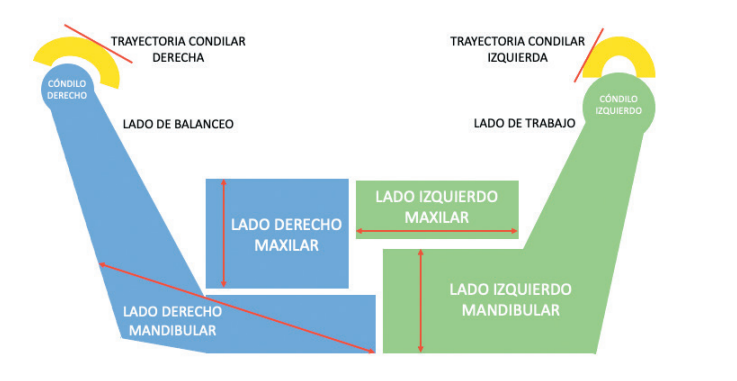
Resultados: La masticación unilateral no alternante genera que la rama mandibular del lado no masticatorio sufra mayor crecimiento debido a que el cóndilo de este lado sólo realiza movimientos de traslación con un enorme estímulo de crecimiento. Además, la mayor carga en el cóndilo del lado de masticación genera cambios anatómicos, encontrándose el cuello engrosado y el área de la cabeza aumentada. Estos cambios a nivel mandibular producen mordida cruzada posterior unilateral en el lado de la masticación con una clase II subdivisión.
Conclusiones: La hiperfunción de los músculos masticatorios y el movimiento mandibular vertical en el lado de la masticación, así como la trayectoria eminentemente traslacional en el lado de balanceo de forma mantenida, genera un crecimiento asimétrico de la mandíbula y de la ATM, desviación del mentón y de línea media dentaria inferior hacia el lado de trabajo, mordida cruzada posterior unilateral y clase II subdivisión en el lado masticatorio, entre otras alteraciones. La terapéutica en etapas tempranas consiste en rehabilitar la función, la aplicación de pistas de composite en el lado cruzado y la expansión maxilar.
Abstract
Introduction: Non-alternating unilateral chewing is a harmful habit consisting of chewing exclusively or predominantly on one of the two sides of the dentition which, maintained over time during growth, causes an asymmetric development of the craniofacial complex, affecting bone structures, muscular, articular and dental.
Aim: Describe how unilateral chewing influences maxillofacial growth and occlusion, as well as the early approach to avoid the consequences of this habit.
Material and method: A bibliographic search was carried out in the EBSCODentistry oral Science Source metasearch engine and in PubMed, selecting full-text articles in English and Spanish related to the subject, of which 45 were extracted to carry out this review.
Results: Non-alternating unilateral mastication causes the mandibular ramus on the non-masticatory side to undergo greater growth because the condyle on this side only performs translational movements with enormous growth stimulus. In addition, the greater load on the condyle on the masticatory side generates anatomical changes, with a thickened neck and an increased head area. These changes at the mandibula level produce a unilateral posterior crossbite on the chewing side with a class II subdivision.
Conclusions: The hyperfunction of the masticatory muscles and the vertical mandibular movement on the chewing side as well as the eminently translational trajectory on the rocking side generates asymmetric growth of the jaw and TMJ, deviation of the chin and midline lower teeth towards the working side, unilateral posterior crossbite and class II subdivision on the masticatory side, among other alterations. Early-stage therapy consists of rehabilitating function, application of composite tracks on the cruciate side, and maxillary expansion.
Este artículo está exclusivamente disponible para su descarga en PDF. | 03/23/2024
Palabras clave
Asimetría mandibular, Maloclusión, Masticación unilateral, Mordida cruzada unilateral
Introducción
El crecimiento y desarrollo del complejo craneofacial es el resultado de la interacción entre factores genéticos y ambientales donde se produce un aumento de tamaño, remodelación y desplazamiento de las estructuras1. Son procesos morfogénicos encaminados hacia un estado de equilibrio funcional y estructural entre todas las partes regionales del tejido duro y blando en crecimiento y desarrollo. Para lograr una oclusión fisiológica, la mandíbula asumirá un mayor crecimiento en longitud que el maxilar1,2.
Los huesos crecen por la aposición de tejido óseo nuevo en un lado de la corteza ósea y resorción en el área opuesta. Este proceso compuesto recibe el nombre de deriva y crea un movimiento directo de crecimiento de cualquier área ósea determinada.
Los determinantes genéticos y funcionales del crecimiento óseo radican en el conjunto de tejidos blandos (músculos, lengua, labios, carrillos, amígdalas, adenoides…) que activan, desactivan, aceleran y retardan las acciones histogénicas de los tejidos conectivos osteógenos1. Durante este crecimiento, los hábitos fisiológicos (habla, deglución normal y masticación) son estímulos para el crecimiento normal de estas estructuras. Sin embargo, existen una serie de hábitos nocivos como la succión digital, la onicofagia, la respiración oral o la interposición lingual que pueden interferir en el desarrollo maxilar y mandibular y ser parte de la etiología de maloclusiones3.
Según la teoría del equilibrio de Proffit, las fuerzas intensas e intermitentes -funcionales- son resistidas por la fisiología, mientras que las fuerzas ligeras y continuas posturales- conducen a unos mecanismos adaptativos que producen remodelación biológica4. Estos hábitos bucales parafuncionales del sistema estomatognático modifican la posición de los dientes y la relación que guardan entre sí, así como el crecimiento normal y la función de la musculatura orofacial, produciendo un desequilibrio entre las fuerzas musculares internas y externas5,6. El diagnóstico precoz de los hábitos anómalos es crucial para la prevención o la corrección temprana de las maloclusiones que se pueden desarrollar6.
Un postulado básico del análisis craneal funcional es que la estructura de la cabeza y el cuello está organizada operativamente en términos de función: digestión, visión, olfato, habla, etc7. Según la hipótesis de las matrices funcionales de Moss, cada una de las funciones se lleva a cabo por un conjunto craneal funcional. Estos componentes están formados por dos partes: una matriz funcional que lleva a cabo la función y una unidad esquelética cuyo papel biomecánico es proteger y/o apoyar su matriz funcional específica. Las unidades esqueléticas son las formadas por hueso, cartílago o tejidos tendinosos. Las matrices funcionales incluyen músculos, glándulas, nervios, vasos, grasa y dientes8.
La masticación unilateral sucede cuando la masticación se realiza constante o predominantemente por uno de los dos lados de la dentición. Tanto la mandíbula como el cóndilo modifican su forma y tamaño si se mantiene el hábito durante el desarrollo9,10. El objetivo de esta revisión bibliográfica es dilucidar los cambios que puede producir la masticación unilateral no alternante durante el desarrollo en las diferentes estructuras del complejo craneofacial, así como determinar las causas por las que se desarrolla este hábito y describir el abordaje precoz durante el crecimiento para la prevención de estas alteraciones.
Bibliografía
Enlow DH. Crecimiento Maxilofacial.
3ª ed. México D.F. Nueva Editorial Interamericana; 1992
Rodríguez-Olivos LHG, ChacónUscamaita PR, Quinto-Argote AG, Pumahualcca G, Pérez-Vargas LF. Deleterious oral habits related to vertical, transverse and sagittal dental malocclusion in pediatric patients. BMC Oral Health 2022;22(1): 88-94.
Muñoz Ruiz J, Kahn S, Ruiz MM y cols. Orthotropics: un sueño hecho realidad. Rev Esp Ortod. 2016;46:108-21.
Ojeda Léonard C, Espinoza Rojo A, Biotti Picand J. Relación entre onicofagia y manifestaciones clínicas de trastornos temporomandibulares en dentición mixta primera y/o segunda fase: Una revisión narrativa. Rev. Clin. Periodoncia Implantol. Rehabil. Oral. 2014;7(1):37-42.
Lorente AA, Cortes O, Guzmán S,
Vicente A, Garrido N. Oral Malocclusion and Its Relation to Nutritive and Nonnutritive Habits in School Children. Open J. Dent. Oral Medicine 2019;7(1):1-8.
Moss ML, Simon MR. Growth of the human mandibular angular process: A functional cranial analysis. Am. J. Phys. Antrophol. 1968;28(2):127-138.
Moss ML, Salentijn L. The primary role of functional matrices in facial growth. Am. J. Orthodontics 1969; 55(6):566-577
Nakano H, Maki K, Shibasaki Y, Miller AJ. Three-dimensional changes in the condyle during development of an asymmetrical mandible in a rat: A microcomputed tomography study. Am J Orthod Dentofacial Orthop. 2004;126(4):410-420.
Ma J, Wang J, Huang D y cols. A comparative study of condyle position in temporomandibular disorder patients with chewing side preference using cone‐beam computed tomography. J Oral Rehabil 2022;49(2):265-271.
Planas P. Rehabilitación Neuro-Oclusal (RNO). 2ª ed. Estrasburgo. Amolca; 2008
Veli I, Uysal T, Ozer T, Ucar FI, Eruz M. Mandibular asymmetry in unilateral and bilateral posterior crossbite patients using cone-beam computed tomography. Angle Orthod. 2011;81(6):966-974.
Jiménez-Silva A, Peña-Durán C, Lee-Muñoz X, Vergara-Núñez C, Tobar-Reyes J, Frugone-Zambra R. Patología temporomandibular asociada a masticación unilateral en adultos jóvenes. Rev. Clin. Periodoncia Implantol. Rehabil. Oral 2016;9(2):125-131
Martinez-Gomis J, Lujan-Climent M, Palau S, Bizar J, Salsench J, Peraire M. Relationship between chewing side preference and handedness and lateral asymmetry of peripheral factors. Arch. Oral Biol. 2009;54(2):101-107
Flores-Orozco EI, Rovira-Lastra B, Peraire M, Salsench J, Martinez-Gomis J. Reliability of a visual analog scale for determining the preferred mastication side. J Prosthet Dent 2016;115(2):203-208
Diernberger S, Bernhardt O, Schwahn C, Kordass B. Self-reported chewing side preference and its associations with occlusal, temporomandibular and prosthodontic factors: results from the population-based Study of Health in Pomerania (SHIP-0). J Oral Rehabil 2008;35(8):613-620.
Facal García A. Diagnóstico y tratamiento precoz de las alteraciones funcionales del desarrollo craneofacial. Ortod Esp. 2006;46(3):79-200.
Larato DS. Effects of unilateral mastication on tooth and periodontal structures. J. Oral Med. 1970;25(3):80-83.
Takada J, Miyamoto JJ, Yokota T, Ono T, Moriyama K. Comparison of the mandibular hinge axis in adult patients with facial asymmetry with and without posterior unilateral crossbite. Eur. J. Orthod 2015;37(1):22-27.
Talapaneni AK, Nuvvula S. The association between posterior unilateral crossbite and craniomandibular asymmetry: A systematic review. J Orthod 2012;39(4):279-291.
Facal García A. Clase II. Forma, función, desarrollo y estabilidad. Expoorto 09. 1ª edición. Varios autores. Editorial Ripano S.A., D. L. 2009:149-168.
Iodice G, Danzi G, Cimino R, Paduano
S, Michelotti A. Association between posterior crossbite, skeletal, and muscle asymmetry: a systematic review. Eur J Orthod 2016;38(6):638-651.
Thilander B, Bjerklin K. Posterior crossbite and temporomandibular disorders (TMDs): need for orthodontic treatment? Eur J Orthod 2011;34(6):667- 673
Anhoury PS. Nonsurgical treatment of an adult with mandibular asymmetry and unilateral posterior crossbite. Am J Orthod Dentofacial Orthop. 2009;135(1):118-126.
Proffit WR. Contemporary Orthodontics. 2ª ed. Michigan. Mosby-Year Book; 1993.
Del Pinal Luna I, Molinero Mourelle P, Torres Loreta L, Bartolomé Villar B. Tratamiento precoz de la mordida cruzada posterior unilateral en el paciente infantil. Revisión bibliográfica. Cient. Dent. 2015;12(3):41-48
Kwak Y, Jang I, Choi D, Cha B. Functional evaluation of orthopedic and orthodontic treatment in a patient with unilateral posterior crossbite and facial asymmetry. Korean J Orthod. 2014;44(3):143-153.
Haralur SB, Majeed MI, Chaturvedi S, Alqahtani NM, Alfarsi M. Association between preferred chewing side and dynamic occlusal parameters. J. Int. Med. Res. 2019;47(5):1908-1915.
Nissan J, Gross MD, Shifman A, Tzadok L, Assif D. Chewing side preference as a type of hemispheric laterality. J Oral Rehabil 2004;31(5):412-416.
Christensen LV, Radue JT. Lateral preference in mastication: a feasibility study. J Oral Rehabil 1985;12(5):421-427.
Tay DK. Physiognomy in the classification of individuals with a lateral preference in mastication. J. Orofac. Pain 1994;8(1):61-72.
Pond LH, Barghi N, Barnwell GM. Occlusion and chewing side preference. J Prosthet Dent 1986;55(4):498-500.
Wilding RJC, Adams LP, Lewin A. Absence of association between a preferred chewing side and its area of functional occlusal contact in the human dentition. Arch. Oral Biol. 1992;37(5):423-438.
Moss ML, DDS. Functional analysis of human mandibular growth. J Prosthet Dent 1960;10(6):1149-1159.
Rogers WM. The influence of asymmetry of the muscles of mastication upon the bones of the facer. Anat. 1958;131(4):617-632.
Legrell PE, Isberg A. Mandibular length and midline asymmetry after experimentally induced temporomandibular joint disk displacement in rabbits. Am J Orthod Dentofacial Orthop. 1999;115(3):247.
Legrell PE, Isberg A. Mandibular height asymmetry following experimentally induced temporomandibular joint disk displacement in rabbits. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998;86(3):280-285.
Marqués Junior JA, J. Lenci PR. Consecuencias de la masticación unilateral en el desarrollo y equilibrio del sistema estomatognático [Internet]. [Consultado 16 Abr 2023].
Disponible en: http://www.labiela.net/La%20Biela01/01jm2.htm
Harvold EP, Francisco C. The role of function in the etiology and treatment of malocclusion.Am. J. Orthod. 1968;54(12):883-898.
Ma J, Wang J, Huang D y cols. A comparative study of condyle position in temporomandibular disorder patients with chewing side preference using cone‐beam computed tomography. J Oral Rehabil 2022;49(2):265-271.
Reinhardt R, Tremel T, Wehrbein H, Reinhardt W. The Unilateral Chewing Phenomenon, Occlusion, and TMD. Cranio 2006; 24(3):166-170.
Santana-Mora U, López-Cedrún J, Mora MJ, Otero XL, Santana-Penín U. Temporomandibular disorders: The habitual chewing side syndrome. PLoS One 2013;8(4):e59980. doi: 10.1371/journal.pone.0059980.
Jiang H, Li C, Wang Z y cols. Assessment of osseous morphology of temporomandibular joint in asymptomatic participants with chewingside preference. J Oral Rehabil 2015;42(2):105-112.
Hinton RJ. Changes in articular eminence morphology with dental function. Am. J. Phys. Anthropol. 1981;54(4):439-455.
Yashiro K, Iwata A, Takada K, Murakami S, Uchiyama Y, Furukawa S. Temporomandibular joint articulations on working side during chewing in adult females with cross-bite and mandibular asymmetry. J Oral Rehabil 2015;42(3):163-172.
Eriksson L, Westesson PL, Macher D, Hicks D, Tallents RH. Creation of disc displacement in human temporomandibular joint autopsy specimens. J. Oral Maxillofac. Surg.1992 50(8):869-873
Pullinger AG, Seligman DA, Gombein JA. A multiple logistic regression analysis of the risk and relative odds of temporomandibular disorders as a function of common occlusal features. J. Dent. Res. 1993; 72(6):968-979.
Petrén S, Bondemark L, Söderfeldt B. A systematic review concerning early orthodontic treatment of unilateral posterior crossbite. Angle Orthod. 2003;73(5):588-596.
De Boer M, Steenks MH. Functional unilateral posterior crossbite. Orthodontic and functional aspects. J Oral Rehabil 1997;24(8):614-623.
Malandris M, Mahoney EK. Aetiology, diagnosis and treatment of posterior cross-bites in the primary dentition. Int J Paediatr Dent. 2004;14(3):155-166.
Brin I, Ben-Bassat Y, Blustein Y y cols. Skeletal and functional effects of treatment for unilateral posterior crossbite. Am J Orthod Dentofacial Orthop. 1996;109(2):173-179.
Petrén S, Bondemark L. Correction of unilateral posterior crossbite in the mixed dentition: a randomized controlled trial. Am J Orthod Dentofacial Orthop. 2008;133(6):790.e7-790.e13. doi. org/10.1016/j.ajodo.2007.11.021.