Revisión bibliográfica
Coronectomía en terceros molares inferiores
La extracción del tercer molar inferior es el procedimiento más frecuente dentro del campo de la cirugía bucal, siendo el daño del nervio dentario inferior una de las complicaciones más frecuentes en la extracción. Como alternativa para disminuir el riesgo de aparición de esta complicación surge la coronectomía, técnica que consiste en la eliminación de la corona dentaria manteniendo intactas las raíces dentro del hueso alveolar. El objetivo del presente artículo fue realizar una puesta al día sobre la coronectomía en terceros molares inferiores, analizando indicaciones, contraindicaciones, complicaciones y éxito de esta técnica.
La coronectomía parece ser una alternativa eficaz a la extracción para la prevención de trastornos neurosensoriales en terceros molares impactados en estrecha relación con el NDI. Sin embargo, es necesaria la realización de más estudios comparando la extracción convencional con la coronectomía, con un mayor seguimiento, para conocer el éxito y las complicaciones a largo plazo de este tratamiento.
The lower third molar extraction is one of the most common procedures in the field of oral surgery. Furthermore, the damage of the inferior alveolar nerve is one of the most frequent complications related to this procedure. The coronectomy was introduced in 1984, as an alternative approach that tended to reduce the occurrence of this complication. The main objective of this article is to review current evidence of coronectomy applied to mandibular third molars, analyzing indications, contraindications, complications and success of the technique.
The coronectomy seems to be an effective alternative to conventional third molar extraction, for the prevention of neurosensorial disorders in impacted third molars in direct relation with inferior alveolar nerve. However, further studies are needed which compare conventional approach with coronectomy with a greater follow-up to understand the long-term morbidities and success of the technique.
Los terceros molares inferiores son los dientes que con más frecuencia se encuentran retenidos en la cavidad oral y, por tanto, su extracción quirúrgica es uno de los procedimientos más habitualmente realizados dentro del campo de la cirugía bucal1 . Esta cirugía conlleva la aparición de la tríada sintomática de dolor, inflamación y trismo en el postoperatorio2 .
Además, existen una serie de posibles complicaciones asociadas a este procedimiento, entre las que se encuentran: la extracción incompleta del diente, daño del segundo molar inferior, desplazamiento del diente a otras regiones anatómicas, fracturas óseas o lesiones neurológicas 3,4. El daño del nervio dentario inferior (NDI) es una de las complicaciones más problemáticas, variando su frecuencia de aparición entre el 0,26% y el 8,4% de los casos3 .
Con el objetivo de disminuir estas complicaciones en casos complejos, se han descrito una serie de alternativas terapéuticas a la extracción, entre las que destaca la coronectomía, cuya técnica fue descrita por primera vez por Ecuyer y Debien en 19845 . Esta técnica consiste en la eliminación de la corona dentaria manteniendo intactas las raíces dentro del hueso alveolar, siendo una alternativa de tratamiento en situaciones en las que las raíces se encuentran en relación íntima con el NDI, reduciendo el riesgo de daño neurológico1 .
El objetivo del presente artículo es realizar una revisión de la evidencia científica actual sobre la técnica de coronectomía en terceros molares inferiores.
La técnica comienza con la elevación de un colgajo vestibular y otro lingual, con el objetivo de exponer el tercer molar inferior y realizar una sección completa de la corona dentaria, previa ostectomía si fuera necesario. La eliminación de la corona debe ser suficiente como para que las raíces remanentes se encuentren como mínimo entre 2 y 3 mm por debajo de la cresta alveolar. Esta medida ha sido consensuada a partir de estudios en animales y ensayos clínicos en los que se ha observado que, al sumergir las raíces a esta profundidad, se favorece el proceso de osteogénesis por encima de las raíces, lo que disminuye el riesgo de una futura migración radicular6-8. Una vez finalizado el proceso de odontosección, es importante comprobar que no exista movilidad en las raíces ni restos de esmalte, dentina o espículas óseas que puedan generar dificultades en la cicatrización y facilitar procesos infecciosos. Para ello, es recomendable regularizar el lecho quirúrgico e irrigar con suero salino o con agentes antisépticos antes de suturar7-9 .
Existen autores que proponen la liberación del periostio del colgajo vestibular para obtener un cierre sin tensión, que permita un aislamiento de la herida y un cierre primario del alveolo. El objetivo fundamental es favorecer el proceso de osteogénesis por encima del resto radicular6 . Las medidas postoperatorias son las habituales tras una cirugía de tercer molar inferior convencional, administrando antibióticos de manera sistémica, analgésicos y antiinflamatorios si fuera necesario. Es muy recomendable también la utilización de antisépticos locales en la herida para evitar la aparición de infección postoperatoria y mejorar la cicatrización7-10 .
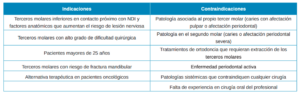
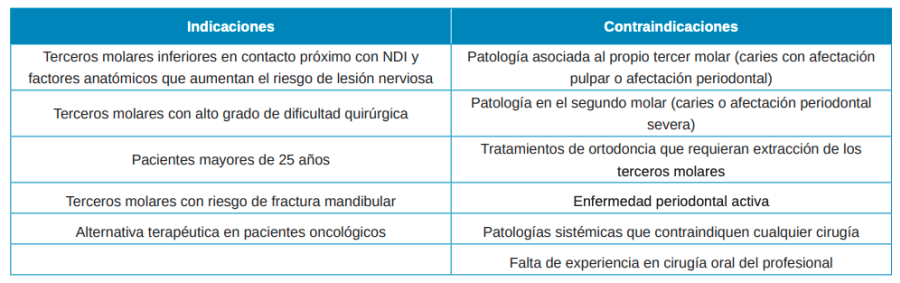
Indicaciones (Tabla 1)
La coronectomía se indica, de manera general, como una técnica alternativa a la extracción de terceros molares inferiores en situaciones en las que, además de haber una causa justificada para la extracción, el diente se encuentre en una posición de proximidad o contacto directo con el conducto del NDI y, por consiguiente, exista un riesgo elevado de dañar el mismo7,8. Para decidir si realizar la extracción convencional u optar por la coronectomía, existen una serie de factores a tener en cuenta:
- Proximidad del NDI: Se han descrito una serie de signos radiológicos en radiografías panorámicas que indican proximidad entre las raíces del tercer molar inferior y el NDI, tales como: interrupción de la línea cortical del conducto dentario inferior, desviación o estrechamiento del conducto y, a nivel de las raíces del tercer molar, oscurecimiento y desviación de éstas. Se ha observado que la incidencia de afectación nerviosa es mayor en los casos en los que aparece el signo de divergencia en el conducto del NDI por la raíz del diente (30%), seguido del oscurecimiento de la raíz (11,6%) y la desviación o curvatura de la raíz producida por el conducto del NDI (4,6%)3 . Szalma y cols.10 observaron una relación significativa entre el signo de curvatura de la raíz y la parestesia postoperatoria, aumentándose el riesgo de desarrollar parestesia en casos en los que la posición de las raíces estuviese en contacto con la cortical del conducto del NDI. En función de las imágenes obtenidas con la radiografía panorámica y debido a sus limitaciones como técnica de imagen bidimensional, estará indicado realizar pruebas radiológicas tridimensionales, como la tomografía computarizada de haz cónico (CBCT), que permitan observar con precisión la posición real del diente y su relación con el NDI.
- Dificultad quirúrgica: En el caso de que el paciente presente un riesgo significativo de daño neurológico, la dificultad quirúrgica es un factor clave a considerar para decidir qué actitud terapéutica llevar a cabo. La dificultad quirúrgica puede ser determinada mediante el índice de dificultad de Pederson, que utiliza la evaluación radiográfica y puntúa de 3 a 10, basándose en: la posición del tercer molar, la profundidad en relación al plano oclusal y la relación con la rama mandibular11, 12 desarrollaron un nuevo índice de dificultad quirúrgica considerando el grado y ángulo de impactación, el número y forma de las raíces, la relación con el conducto del NDI y la edad del paciente. En función de estos criterios se obtiene una puntuación que determina la dificultad quirúrgica. Así, en casos de relación íntima del tercer molar con el NDI y con una alta dificultad quirúrgica, se valorará como alternativa terapéutica a la extracción la coronectomía.
- Edad del paciente: La edad del paciente se ha considerado un factor determinante para el nivel de dificultad quirúrgica de la extracción del tercer molar inferior, aumentando la dificultad en pacientes a partir de 25-35 años12 . Además, se ha observado una menor tasa de recuperación neurológica en pacientes mayores tras la cirugía del tercer molar7 . Por ello, esta técnica se recomienda generalmente en pacientes mayores de 25 años.
- Riesgo de fractura mandibular: La fractura mandibular es una de las complicaciones asociadas a la cirugía del tercer molar, con una frecuencia del 0,045%13. Suele ocurrir en casos de terceros molares retenidos muy profundos, con perforación o afectación de corticales y habitualmente en pacientes de unos 30-40 años. En estos casos, la coronectomía puede ser una alternativa eficaz para evitar el riesgo de fractura mandibular.
- Pacientes oncológicos: Todos los pacientes que vayan a ser sometidos, tanto a radioterapia de cabeza y cuello como a quimioterapia por patología oncológica, siempre requieren una valoración del estado bucodental previo, para evitar complicaciones durante el tratamiento y eliminar posibles focos sépticos. En casos de pacientes que requieran tratamiento oncológico y presenten terceros molares susceptibles de dar patología o terceros molares sintomáticos en relación estrecha con NDI o alta dificultad quirúrgica, la coronectomía se ha propuesto como una posible alternativa de tratamiento para disminuir las complicaciones que pueden surgir de una extracción quirúrgica convencional durante el tratamiento del paciente oncológico14 .
de coronectomía.
Así, en función de estos factores se pueden establecer una serie de indicaciones generales:
- Terceros molares inferiores en contacto íntimo con el NDI y con factores anatómicos que aumenten el riesgo de lesión nerviosa, como la curvatura acentuada de las raíces.
- Terceros molares con alto grado de dificultad quirúrgica que aumenten los riesgos de la extracción.
- Pacientes mayores de 25 años.
- Terceros molares con riesgo de fractura mandibular
- Alternativa terapéutica en pacientes oncológicos.
Contraindicaciones (Tabla 1)
Las contraindicaciones para la realización de la técnica de coronectomía incluyen la presencia de: 1) Patología asociada al propio tercer molar (infección periapical, caries con afectación pulpar o radicular, pericoronaritis, movilidad y patología quística/tumoral asociada); 2) Patología en el segundo molar (caries o afectación periodontal severa); 3) Tratamientos de ortodoncia que requieran extracción de los terceros molares; 4) Enfermedad periodontal activa; 5) Patología o condición sistémica del paciente que suponga una contraindicación extensible a cualquier otra cirugía (tratamiento con radioterapia o quimioterapia, tratamiento con fármacos antirresortivos, diabetes mal controlada, enfermedades infecciosas, hepatitis, alcoholismo, tabaquismo, drogadicción); 6) Falta de experiencia del profesional en cirugía oral9 .
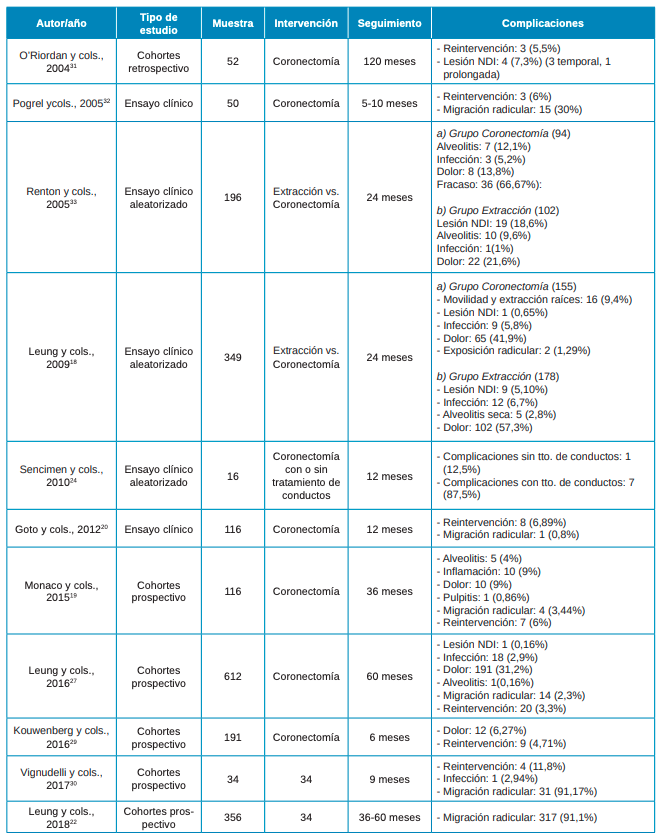
Complicaciones (Tabla 2)
Del mismo modo que tras la cirugía convencional del tercer molar, la coronectomía cursa con la triada típica de dolor, trismo e inflamación inherente al acto quirúrgico2 .
Según la evidencia actual, no se observan diferencias estadísticamente significativas entre coronectomía y extracción completa en cuanto a dolor, trismo e inflamación. Sin embargo, se han registrado menores tasas de dolor postoperatorio e coronectomía en comparación con la extracción completa12, 15, 16 .
En cuanto al riesgo de lesión nerviosa, parece ser mayor en la cirugía de extracción del tercer molar inferior que tras la coronectomía. En el estudio de Leung y Cheung3 se obtuvo un 0,16% de casos con déficit neurosensorial, en pacientes tratados con coronectomía, mientras que el porcentaje de lesión nerviosa tras la cirugía del tercer molar suele oscilar entre 0,3% y 3,0%. Por otro lado, Long y cols.17 observaron que el riesgo relativo de daño neurológico en pacientes sometidos a extracción completa en comparación con coronectomía es de 0,11%, lo que supone unas 10 veces más de probabilidades de sufrir un déficit neurosensorial en comparación con los pacientes tratados con coronectomía.
La aparición de alveolitis durante la primera semana se ha observado en un rango de porcentajes bajos en pacientes tratados con coronectomía, entre un 0% y un 0,16%15,18. En comparación con la extracción completa, donde aparece de manera más frecuente, Leung y cols.,18 en 2009 obtienen un 2,8% de casos con alveolitis frente al 0% en el grupo de pacientes tratados con coronectomía.
De manera específica aparecen una serie de complicaciones derivadas de la coronectomía, generalmente tardías, entre las que se encuentra la necesidad de reentrada debido a migración de las raíces, con un rango de entre el 13,2% y el 85,29%. Este suceso puede considerarse en cierto modo favorable, ya que permite a posteriori la completa extracción del diente en caso de que la migración se haya producido en dirección coronal. Goto y cols.,20 observaron que tanto la edad, como el sexo y la morfología radicular son factores correlacionados con la migración radicular, siendo ésta mayor en pacientes jóvenes y en mujeres. Se observa un aumento de la migración radicular desde el primer día hasta 6 meses después de la cirugía, produciéndose el efecto migratorio en mayor medida durante los primeros 6 meses16,17,19-21. En el estudio de Leung y cols.,22, se analizaron los patrones de migración de las raíces como una complicación tardía del tratamiento en coronectomías y se observó una migración radicular en la práctica totalidad de los casos tratados (91%), variando claramente la proporción de casos en función del tiempo. Determinaron que, a partir de los 6 meses de seguimiento, la cantidad de raíces migradas disminuye, hasta el 24% a los 2 años y hasta el 4% a los 5 años. En este mismo periodo de observación, se determinó que la posición inicial del cordal influye en su posible migración radicular, de forma que aquellos cordales con una posición distoangular presentan una menor incidencia de migración radicular frente al resto de posiciones anatómicas. No obstante, para interpretar estos resultados, hay que considerar que la posición distoangular en terceros molares es la menos prevalente22 .
Otra complicación derivada de la técnica de coronectomía es la aparición tardía de infección, debido a la incorrecta eliminación del esmalte residual23 .

Tratamiento endodóntico de los restos radiculares
La aparición de complicaciones asociadas a infección causada por el resto radicular y, en especial, por el tejido pulpar residual, sujeto a una necrosis a lo largo del tiempo, ha llevado a la discusión de si es conveniente o no la realización de tratamientos de conductos en los restos radiculares22, 23, 24 .
Sencimen y cols.,24 evaluaron el efecto del tratamiento de conductos. Se llevaron a cabo 16 coronectomías, realizando tratamiento de conductos en 8 de ellas. Los resultados revelaron que, en 7 casos, las raíces tuvieron que ser extraídas por infección después del procedimiento, y 3 de los pacientes presentaron parestesia temporal del NDI, atribuyendo estos resultados al aumento en la duración de la intervención. Estudios previos sugieren que la realización de tratamiento de conductos en las raíces remanentes parece no proporcionar ningún beneficio añadido a la técnica de coronectomía, pero sí podría incrementar el riesgo de aparición de complicaciones infecciosas25,26 .
Regeneración en coronectomía
La regeneración ósea guiada (ROG) se ha propuesto como tratamiento complementario tras la técnica de coronectomía, con el objetivo de regenerar el defecto provocado al realizar la extracción parcial del tercer molar y así, reducir la migración radicular coronal y la aparición de defectos óseos en distal del segundo molar.
Leung ycols.,27 en 2016 realizaron ROG con hueso bovino y membrana reabsorbible tras la coronectomía y observaron una disminución de la migración radicular en comparación con las tasas habituales sin realizar ROG. En otro estudio del mismo autor en 2019, se comparó la coronectomía con o sin ROG con un seguimiento de 24 meses, observando diferencias estadísticamente significativas en cuanto a migración radicular a favor del grupo con ROG28 .
Por tanto, la ROG después de la técnica de coronectomía parece disminuir la tasa de migración radicular.
Reintervención tras la coronectomía
Barcellos y cols.,23 realizaron una revisión sistemática, cuyo objetivo era la descripción de los parámetros que indican la necesidad de una segunda intervención en los pacientes sometidos a coronectomía. Concluyeron que las situaciones que precisan reintervención tras la coronectomía son:
a) Migración radicular: Un 30% de las raíces migran hasta 4 mm los dos primeros años y, en un 82,2%, ésta se detiene a partir del segundo año. Sin embargo, aunque se produzca la migración, en la mayoría de los casos las raíces permanecen asintomáticas y cubiertas por hueso. Sólo se considera motivo de reintervención la exposición de los restos radiculares, con el fin de evitar las complicaciones inflamatorias23,29 .
b) Dolor: Los pacientes pueden presentar dolor asociado a la propia intervención durante la primera semana. Si el dolor persiste, habitualmente suele ser debido a inflamación del tejido pulpar remanente en el resto radicular o a una infección del lecho. En esos casos, y dependiendo de la evolución, será necesaria o no la reintervención, aunque no existen protocolos sobre cuándo debe realizarse19,23,29,30 .
c) Infección: Basándonos en los estudios revisados, no parecen existir diferencias significativas entre pacientes sometidos a coronectomía o a extracción completa del tercer molar inferior en cuanto a la aparición de infección. Es difícil de predecir, ya que está relacionado con la respuesta fisiopatológica del individuo y la higiene oral. En este sentido, realizar una técnica incorrecta de coronectomía, dejando espículas de esmalte en la cavidad puede ser una de las causas principales de infección23 .
En el estudio de Leung y cols.,15 en 2016 se observa un porcentaje de reintervención en un 3,3% de los casos: un 0,49% fue debido a infección, un 2,1% debido a exposición radicular, un 0,49% por dolor en la zona mandibular posterior y un 0,16% por incompatibilidades de diferentes tratamientos (cirugía ortognática). En otro estudio de Leung y cols.,18, se observa un 1,16% de reintervenciones, debido a infección. Martin y cols.,8 consideran un porcentaje de reintervención debido a la migración radicular o infecciones de entre 0,6% y 6,8%. Dentro de ese rango se encuentra el estudio de O’Riordan y cols.,31, en el cual el porcentaje de reintervención es de un 5,76% debido a infección y migración coronal de las raíces.
Fracaso
Las tasas de fracaso observadas en los estudios varían de un 0%19,20,31 a un 38,3%32. Sin embargo, existen diferentes conceptos de éxito y fracaso en la técnica de coronectomía. Algunos investigadores consideran el fracaso la necesidad de reintervención debido a infección18,32. Otros, consideran fracaso en la técnica la necesidad de extracción completa del diente debido a la movilización de las raíces durante el proceso de odontosección coronal8, 19 . Por tanto, se hace necesaria la unificación de criterios de éxito y de fracaso para poder esclarecer la verdadera eficacia de esta técnica.
Seguimiento
El seguimiento del paciente en esta técnica es crucial para poder detectar complicaciones manera precoz y prevenirlas. Se considera que la lesión nerviosa puede aparecer en un periodo de hasta 25 meses y la erupción tardía, debido a la migración radicular, puede ocurrir en un periodo más largo de tiempo, con lo cual el seguimiento ha de ser a largo plazo, realizando radiografías panorámicas como mínimo cada 2 ó 3 años8 .
Debido a que los estudios que mayor seguimiento presentan son a 10 años, todavía no se han establecido protocolos clínicos de seguimiento. Por tanto, se consideran necesarios estudios con un mayor seguimiento a largo plazo mediante los cuales se puedan establecer protocolos estandarizados firmes al respecto.
La coronectomía se considera una alternativa eficaz a la extracción para la prevención de trastornos neurosensoriales en terceros molares retenidos con indicación de extracción y en estrecha relación con el NDI. Sin embargo, no es una técnica exenta de complicaciones, siendo las más frecuentes la infección, el dolor postoperatorio y la migración radicular. Existe una falta de homogeneidad en los criterios de éxito, fracaso, protocolos de tratamiento y seguimiento. Por tanto, se hacen necesarios estudios clínicos aleatorizados comparando la extracción convencional con la coronectomía, con un mayor seguimiento, para conocer el éxito y las complicaciones a largo plazo de este tratamiento.

Encinas Ramos, Ana
Alumna del Máster en Ciencias Odontológicas. Universidad Complutense de Madrid (UCM).
Sáez-Alcaide, Luis Miguel
Máster en Cirugía Bucal e Implantología. Universidad Complutense de Madrid.
Cobo-Vázquez, Carlos
Profesor colaborador honorífico. Departamento de Especialidades Clínicas Odontológicas. Facultad de Odontología (UCM).
Meniz García, Cristina
Profesora Contratada Doctor. Departamento de Especialidades Clínicas Odontológicas. Facultad de Odontología (UCM).
Indexada en / Indexed in: – IME – IBECS – LATINDEX – GOOGLE ACADÉMICO